Downloaded 279 times
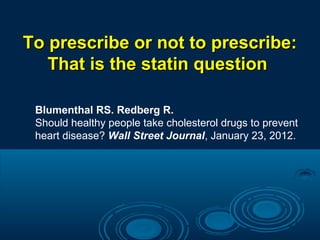
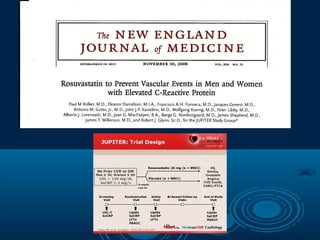
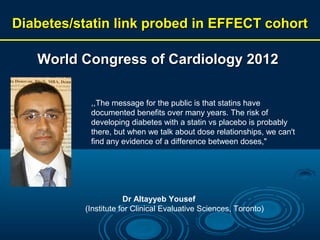
![Diabetes Care
October 2009; vol. 32: no.10: 1924-1929
Statin Therapy and Risk of Developing
Type 2 Diabetes: A Meta-Analysis
Swapnil N. Rajpathak, Dharam J. Kumbhani, Jill Crandall,
Nir Barzilai, Michael Alderman, Paul M. Ridker.
RESULTS
In the meta-analysis of the hypothesis-testing trials,
we observed a small increase in diabetes risk
(RR 1.13 [95% CI 1.03–1.23])](https://image.slidesharecdn.com/statinelesidiabetulzaharat-131110001216-phpapp01/85/Statins-and-diabetes-risk-12-320.jpg)
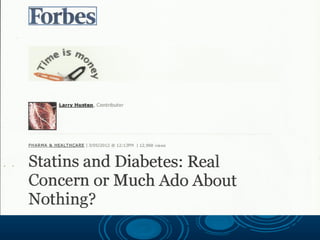
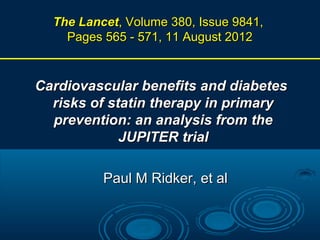
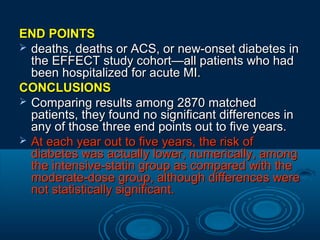
![Results
In 5 statin trials with 32.752 participants without diabetes at
baseline, 2749 developed diabetes (1449 assigned intensive-dose
therapy, 1300 assigned moderate-dose therapy, representing 2.0
additional cases in the intensive-dose group per 1000 patientyears) and 6684 experienced cardiovascular events (3134 and
3550, respectively, representing 6.5 fewer cases in the intensivedose group per 1000 patient-years) over a weighted mean (SD)
follow-up of 4.9 (1.9) years.
Odds ratios were 1.12 (95% confidence interval [CI], 1.041.22; I2 = 0%) for new-onset diabetes and 0.84 (95% CI, 0.750.94; I2 = 74%) for cardiovascular events for participants receiving
intensive therapy compared with moderate-dose therapy.
As compared with moderate-dose statin therapy, the number
needed to harm per year for intensive-dose statin therapy was 498
for new-onset diabetes while the number needed to treat per year
for intensive-dose statin therapy was 155 for cardiovascular events.
Conclusion: In a pooled analysis of data from 5 statin trials, intensivedose statin therapy was associated with an increased risk of new-onset
diabetes compared with moderate-dose statin therapy.](https://image.slidesharecdn.com/statinelesidiabetulzaharat-131110001216-phpapp01/85/Statins-and-diabetes-risk-16-320.jpg)
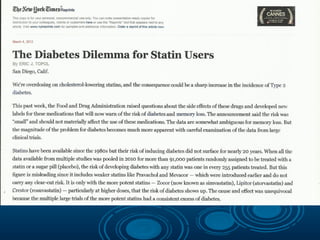
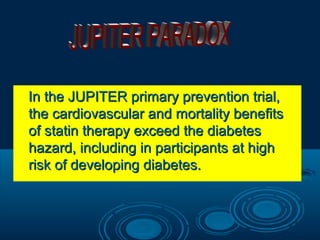
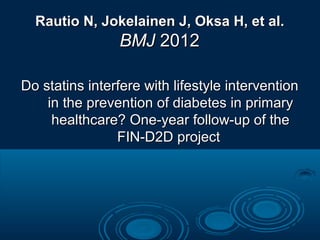
![13 statin trials
91.140 participants, of whom 4278 (2226 assigned statins and 2052
assigned control treatment) developed diabetes during a mean of 4
years.
Statin therapy was associated with a 9% increased risk for incident
diabetes (odds ratio [OR] 1·09; 95% CI 1·02—1·17), with little
heterogeneity (I2=11%) between trials.
Meta-regression showed that risk of development of diabetes with
statins was highest in trials with older participants, but neither
baseline body-mass index nor change in LDL-cholesterol
concentrations accounted for residual variation in risk.
Treatment of 255 (95% CI 150—852) patients with statins for 4
years resulted in one extra case of diabetes.
Interpretation
Statin therapy is associated with a slightly increased risk of
development of diabetes, but the risk is low both in absolute terms
and when compared with the reduction in coronary events.
Clinical practice in patients with moderate or high
cardiovascular risk or existing cardiovascular disease should
not change.
Sattar N et al. Lancet 2010](https://image.slidesharecdn.com/statinelesidiabetulzaharat-131110001216-phpapp01/85/Statins-and-diabetes-risk-20-320.jpg)
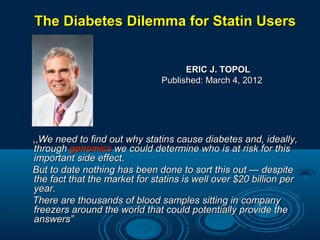
![
Results
This investigation included 153 840
women without DM and no missing
data at baseline. At baseline, 7.04%
reported taking statin medication.
There were 10 242 incident cases of
self-reported DM over 1 004 466
person-years of follow-up.
Statin use at baseline was associated
with an increased risk of DM (hazard
ratio [HR], 1.71; 95% CI, 1.61-1.83).
This association remained after
adjusting for other potential
confounders (multivariate-adjusted
HR, 1.48; 95% CI, 1.38-1.59) and was
observed for all types of statin
medications.
Conclusions
Statin medication use in
postmenopausal women is
associated with an increased
risk for DM.
This may be a medication
class effect.
Further study by statin type
and dose may reveal varying
risk levels for new-onset DM in
this population.
Subset analyses evaluating the
association of self-reported DM with
longitudinal measures of statin use in
125 575 women confirmed these
findings.
Arch Intern Med. Published online January 9, 2012](https://image.slidesharecdn.com/statinelesidiabetulzaharat-131110001216-phpapp01/85/Statins-and-diabetes-risk-23-320.jpg)

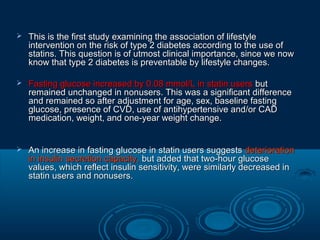
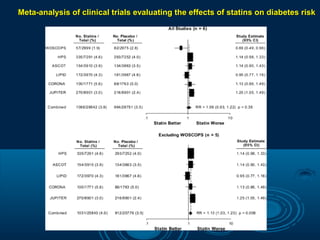
![Kaplan-Meier Curves for Outcomes
Among Statin and Control Groups
(A) Cumulative incidences for newly developed
diabetes in the statin and control groups
were 22.7% and 20.8%, respectively.
(B) Cumulative incidences for major adverse
cardiovascular (CV) events (the composite
of myocardial infarction [MI] and ischemic
stroke) in the statin and control groups
were 11.6% and 12.6%,
(C) Cumulative incidences for in-hospital death
from all causes in the statin and control
groups were 8.8% and 13.8%.
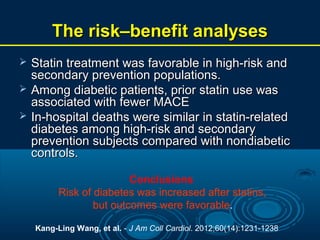
Kang-Ling Wang, et al. - J Am Coll Cardiol. 2012;60(14):1231-1238.](https://image.slidesharecdn.com/statinelesidiabetulzaharat-131110001216-phpapp01/85/Statins-and-diabetes-risk-35-320.jpg)
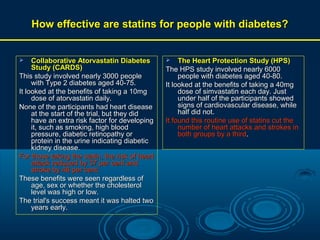


Statin use is associated with a small increased risk of developing diabetes. However, the cardiovascular benefits of statin therapy still outweigh the diabetes risk. Several studies have found that statin use leads to a 9-13% increased risk of diabetes, but the absolute increased risk is low. The number of patients needed to treat with statins to prevent a cardiovascular event is lower than the number needed to harm in terms of diabetes risk. Therefore, clinical practice for statin therapy for reducing cardiovascular risk should not change.























































































