


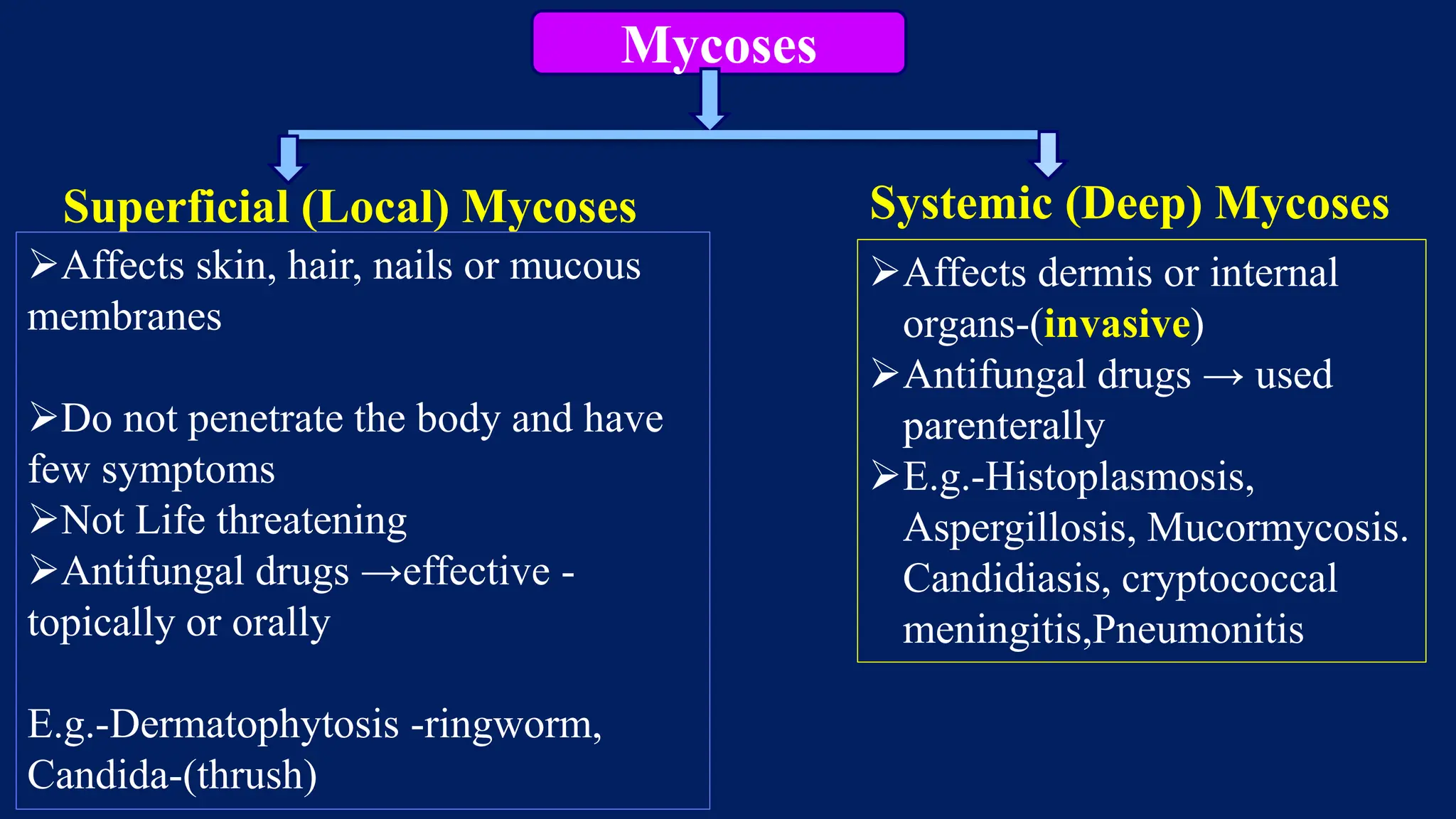




























This document summarizes common fungal infections and the antifungal drugs used to treat them. It discusses both superficial and systemic mycoses caused by fungi like Candida, Dermatophytes, Aspergillus, and Cryptococcus. The main classes of antifungal drugs covered are polyenes like amphotericin B and nystatin, azoles including imidazoles and triazoles, antimetabolites like flucytosine, and allylamines such as terbinafine. Specific drugs discussed in detail include amphotericin B, griseofulvin, ketoconazole, fluconazole, itraconazole, voriconaz























































































