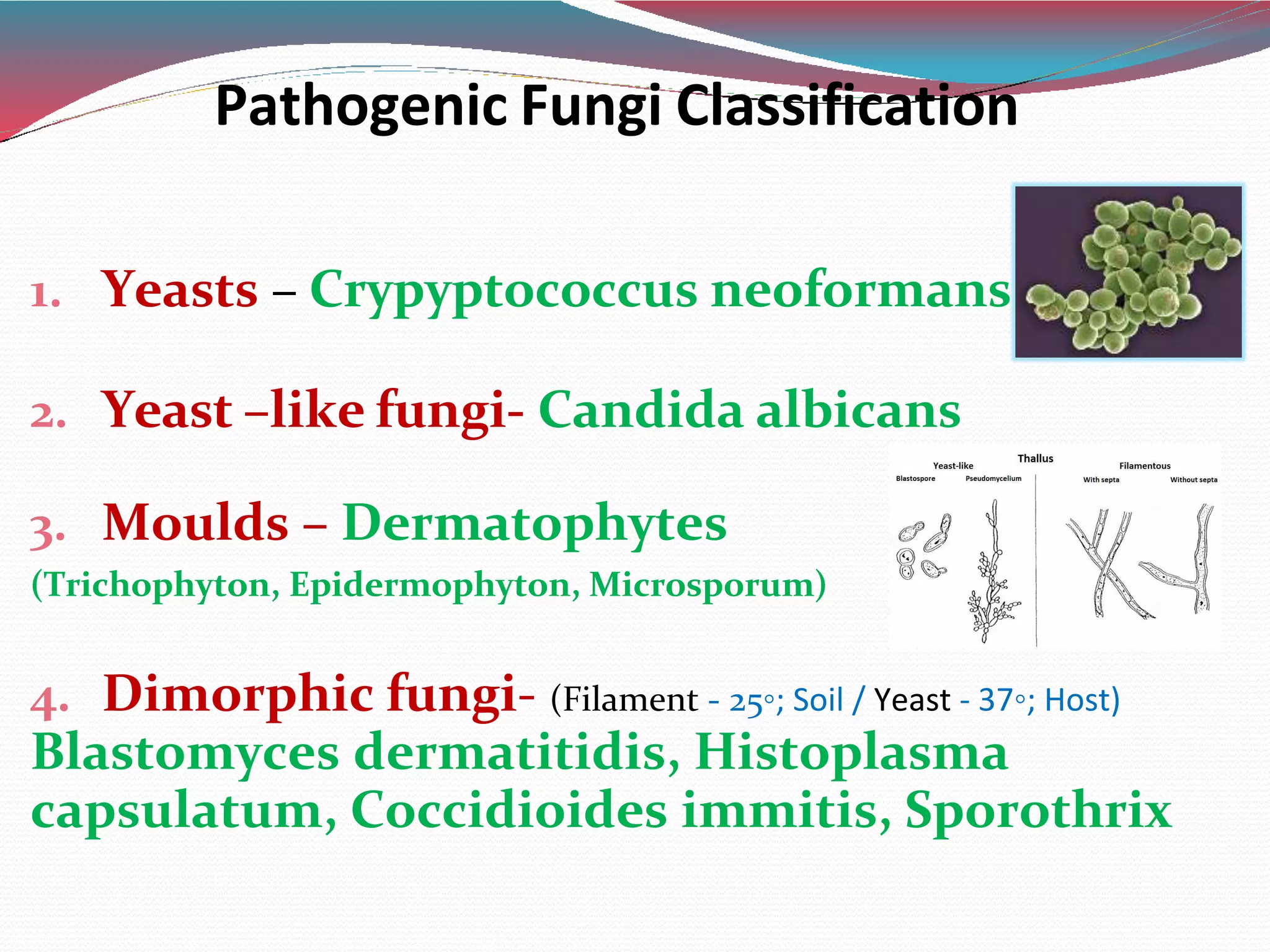
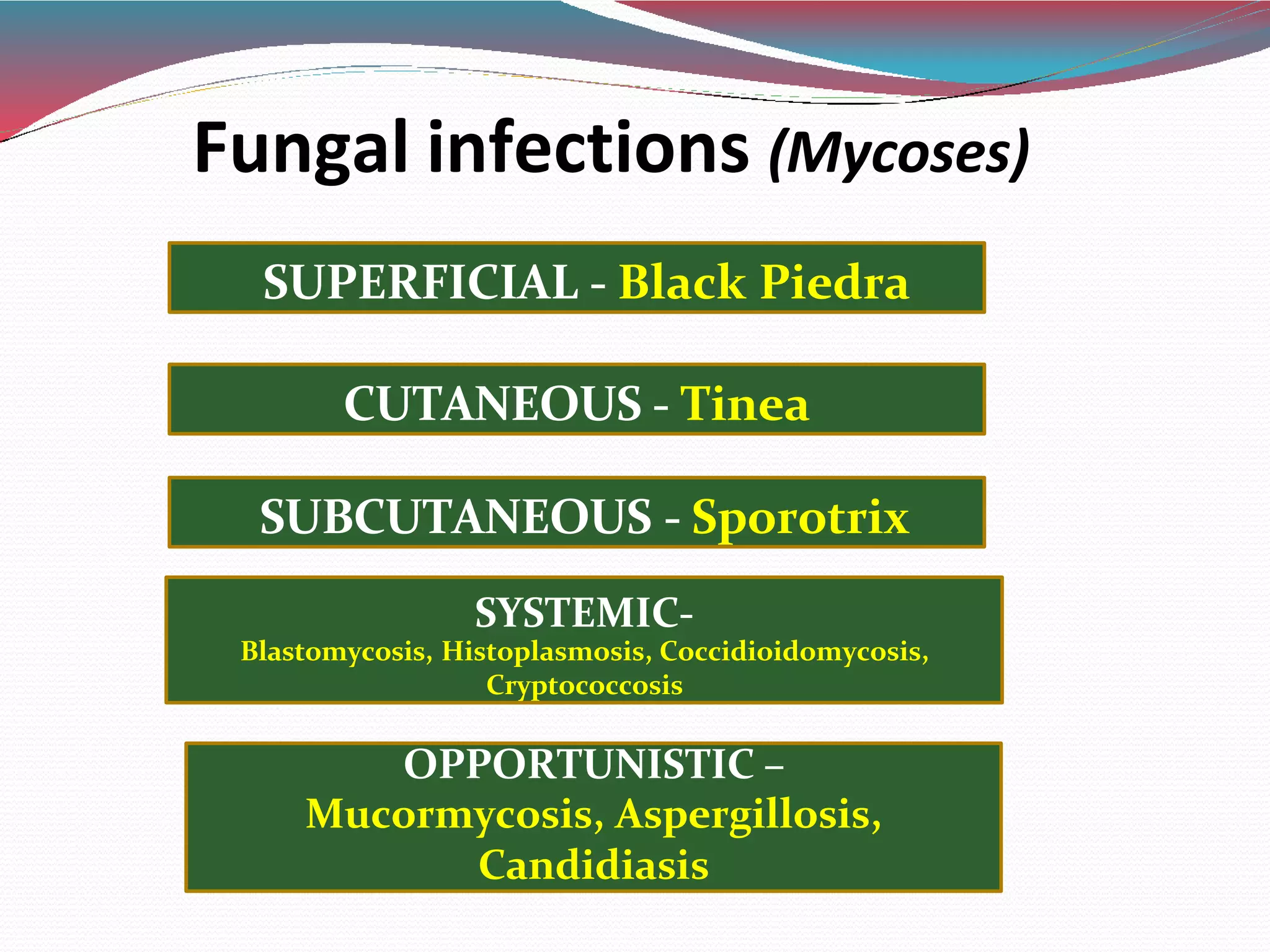
This document provides a classification and overview of pathogenic fungi and antifungal drugs. It begins by classifying fungi into yeasts, yeast-like fungi, molds, and dimorphic fungi. It then categorizes fungal infections as superficial, cutaneous, subcutaneous, or systemic/opportunistic. The document further discusses the classification, mechanisms of action, pharmacokinetics, uses, and adverse effects of various antifungal drug classes including polyenes, azoles, allylamines, echinocandins, and others. It provides details on specific drugs like amphotericin B, nystatin, ketoconazole, fluconazole, itraconazole,