Download to read offline

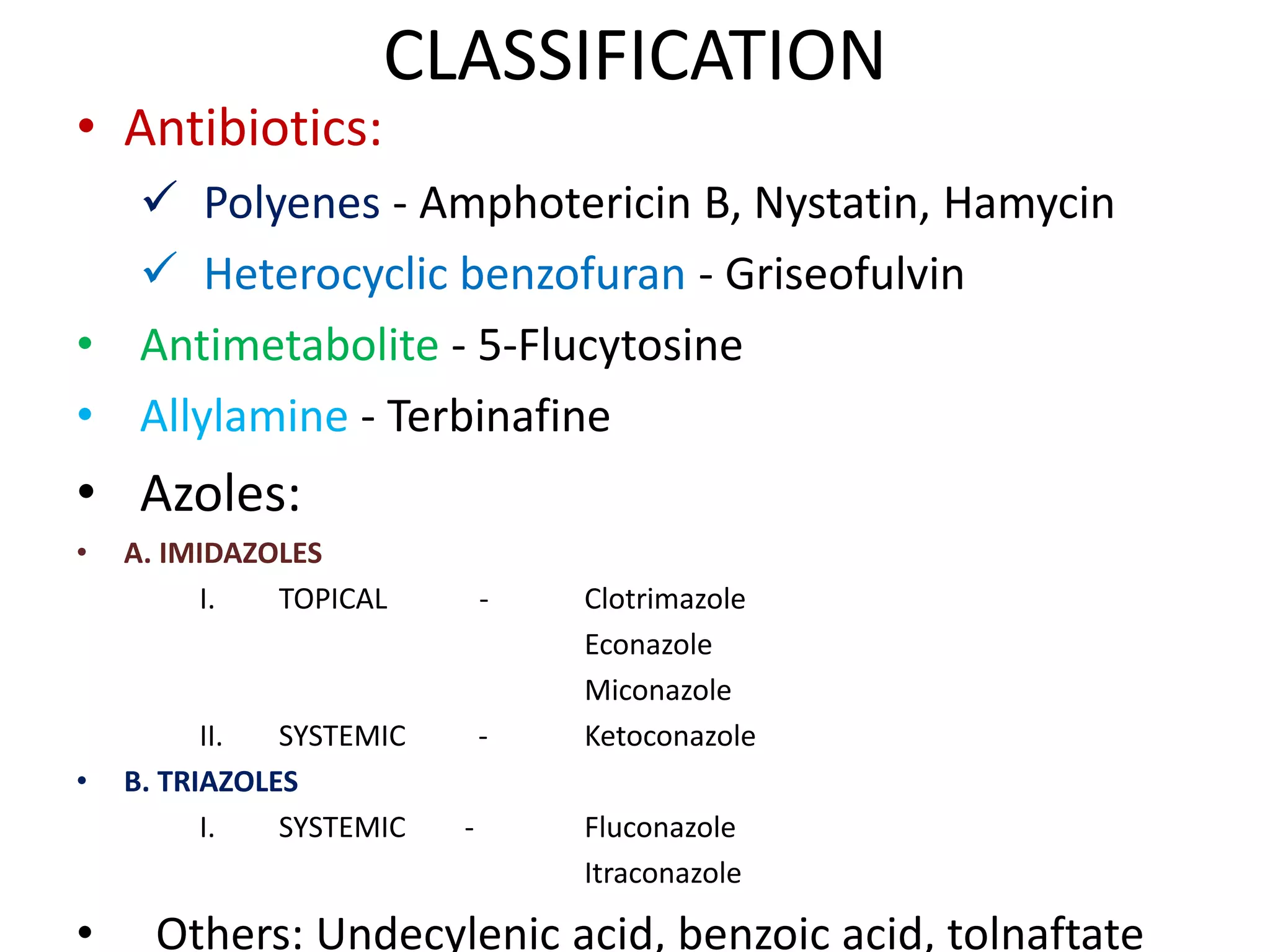


















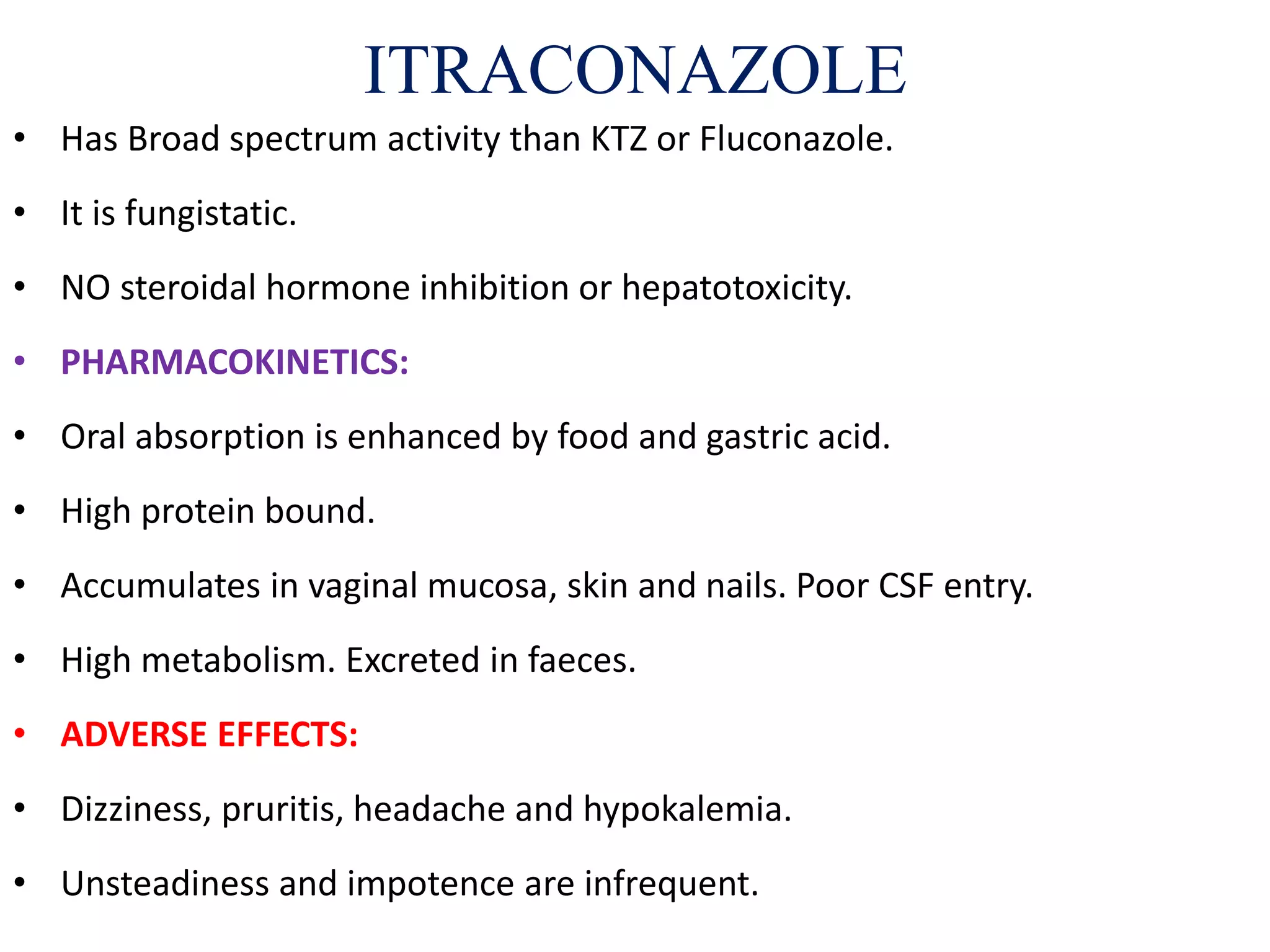





This document provides an extensive overview of various antifungal agents, categorizing them into classes such as polyenes, azoles, and allylamines, detailing their mechanisms of action, pharmacokinetics, and clinical uses. It outlines the effectiveness and side effects of drugs like griseofulvin, amphotericin B, ketoconazole, fluconazole, itraconazole, and terbinafine among others, as well as their interactions and dosing regimens. It emphasizes the selective toxicity of these agents against specific fungi while noting their limited efficacy against some strains, including Candida.



































































