Introduction
o Def:- Adrug-induced reversible loss of consciousness where patients
cannot be aroused, even by painful stimulation.
General anesthesia is used during surgical operations to produce:
– Reversible Loss of consciousness
– Reversable loss of sensation
– Analgesia & Amnesia
– Skeletal muscle relaxation
General An aesthesia
All over the body No Sensation
All effect cant be
achieved by single
agents
Balanced anaesthesia
Combination of general anesthetics
lesser toxicity
↓dose of individual agents
Anaesthetic protocol include
1.Premedication
2.Induction of anaesthesia (e.g. thiopentone and propofol).
3. Maintenance of anaesthesia (N2O + Isoflurane/Halothane).
4. Skeletal muscle relaxation.
5. Analgesia—as Premedication, during and after the operation.
6. Use of other drugs:-
To reverse neuromuscular blockade.
To reverse the residual effects of opioids (naloxone) and
BZDs (flumazenil).
To achieve all the objectives of anaesthesia by using of appropriate
preanesthetic medication, inducing agents, muscle relaxant, analgesic
with suitable General anesthetic Agents is called balanced anaesthesia
5.
Ideal Anesthetic Management
•Hypnosis and amnesia
• Block reflex reactions to pain
• Provide skeletal muscle paralysis
• Maintain vital functions
• Rapid & smooth induction of anesthesia
• Physical safety
6.
Stages of GeneralAnaesthesia
Stage-I (Stage of Analgesia)- start from beginning of
anaesthetic inhalation upto -loss of consciousness
Pt.- conscious but drowsy (Minor procedure can be perform in this
stage)
Stage-II (Stage of Excitement):- (loss of consciousness)
Start from loss of consciousness to beginning of regular respiration
↑Sympathetic activity -↑HR,↑BP, pupils are dilated, ↑ muscle tone,
Irregular jerky breathing, patient may shout, struggle and hold his
breath, jaws are tightly closed
No operative procedure should be carried out in this stage
Stage-III (Stage of Surgical anaesthesia):-
All surgical procedure are performed in this stage
The aim of induction is to reach stage-III as early as possible followed
by maintenance anaesthesia and muscle relaxation
7.
Respiration becomes regular,Muscles relax, Reflexes are
gradually lost, Intercostal muscles are paralysed
Consist of 4 plane-
1.Plane-1:-Roving eyeballs. This plane ends when eyes
become fixed
2. Plane-2 (Loss of corneal and laryngeal reflexes)
3. Plane-3 (Pupil starts dilating and light reflex is lost)
4. Plane-4(intercostal paralysis, shallow abdominal
respiration, dilated pupil)
8.
Stage-IV:- (Stageof medullary paralysis)
Due to overdose
Depression-RC & VMC
Death occurs within a few minutes
Mechanism of Action:-
Site of Action- Reticular formation (maintains consciousness)
Most anesthetics depress reticular formation by enhancing
the activity of inhibitory transmitters and blocking the
activity of excitatory transmitters
Minimum Alveolar Concentration(MAC)
• Minimum concentration of anesthetic in alveoli that is
required to prevent movement in 50% of patients in
response to a surgical incision.
• It indicate- potency of Anesthetics
• Low MAC means=high potency=↑lipophilicity
• Expressed as percentage
• Age dependent-Highest-infants
• High MAC value-low Blood solubility-↑Diffusion-
↑Anaesthetic induction & recovery
E.g.- N20(105%)-least potent. Halothane(0.75%)-maximum
Potency
Pharmacokinetic properties of GA:-
11.
Factor affecting MAC
Factorto decrease MAC:-
Hypotension,
Anemia,
Hypothermia,
Metabolic acidosis,
Hypoxia,
Pregnancy,
Aging,
Hypothyroidism,
Recurrent use of Analgesic
Factor to increase MAC:-
↑Body temp
Hyperthyroidism,
Hypernatremia
12.
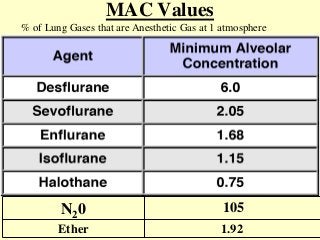
MAC Values
% ofLung Gases that are Anesthetic Gas at 1 atmosphere
N20 105
Ether 1.92
13.
• N20- lowblood solubility hence rapidly diffuses to brain and
produce rapid induction of Anaesthetic action followed by recovery.
• Where as halothane/isoflurane- poorly diffuse followed by slow
induction of Anaesthetic action & recovery
• Hence, combination of (N20 + Halothane/isoflurane)
Second Gas effect
↑↑Diffusion rate of halothane/isoflurane
(Rapid induction of Anaesthetic action)
Advantage:-
Low dose can produce anesthetic effect
Less toxicity of halothane/isoflurane-like hypotension, RS depression
Due to low dose-recovery will be faster
Halothane/isoflurane -potent anaesthetic and poor analgesic
N2O is a good analgesic and poor anaesthetic
Combined effect -potent anaesthesia with good analgesia.
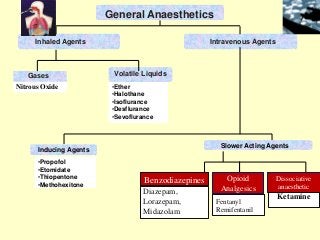
14.
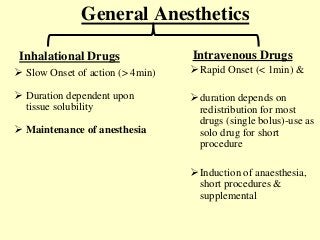
General Anesthetics
Intravenous Drugs
RapidOnset (< 1min) &
duration depends on
redistribution for most
drugs (single bolus)-use as
solo drug for short
procedure
Induction of anaesthesia,
short procedures &
supplemental
Slow Onset of action (> 4min)
Duration dependent upon
tissue solubility
Maintenance of anesthesia
Inhalational Drugs
15.
Inhalational Anesthetics
• Thereare two physical forms
– Gases:-
• Supplied in gas tanks for delivery by anesthesia machine
• N2O is only one currently in use
– Volatile liquids:-
• Delivered by vaporizers attached to anesthesia machine
• Several halogenated hydrocarbon volatile anesthetics exist
• Ether, halothane, enfluroane, isoflurane, desflurane, sevoflurane
16.
Individual Agents:- NitrousOxide
• Colorless, Sweetish odor-known for Laughing Gas
• Non-irritating, Non-inflammable, Non-explosive-Gaseous
general anesthetic agent.
• Not metabolized in body
• Mostly eliminated unchanged through lungs(95%) & 5%
through skin
• Low efficacy anaesthetic agent-possible by blocking
NMDA receptor
• 15 time more soluble than 02 & 35 time more soluble than
nitrogen
• Light anesthesia without significant depression of RS &
CVS
17.
• :
Advantages Disadvantages
Goodanalgesic
Rapid and smooth induction-low
blood solubility
Non irritating and non-
inflammable
Rapid recovery
Non toxic to liver, kidney and
brain
Inexpensive
Post anesthetic nausea less
Negligible effect on CVS &
Respiratory system
Acts as a carrier gas to other
agents
Less potent
Not a good anaesthetic
Low efficacy due to high MAC
value
Not a muscle relaxant
↑intracranial tension
18.
• Diffusion hypoxia:-Discontinued of N2O while
recovery from anesthesia leading to ↑diffusion from
blood to alveoli causes marked ↓ PaO2 resulting in
hypoxia, which is known as diffusion hypoxia.
Rx-100% O2 administered for a few minutes
Immediately after N2O is discontinued.
Prolong use-Agranulocytosis-interfere with folate
metabolism & impairs DNA synthesis
Megaloblastic anemia-Due to inactivation of Vit-
B12 component(cobalamin)
Laryngospasm & methemoglobinemia
Side effect:-
19.
Ether
Highly inflammable& irritant , volatile, explosive vapor
with pungent smell
Decompose to light, air & heat(store in dark bottle)
Advantages Disadvantages
Potent and reliable
Good analgesic
Good muscle relaxant
Doesn't sensitize heart to
adrenaline
Easy to administer and
inexpensive
Less expensive
Induction slow and unpleasant
Irritating and ↑salivation & resp
secretions-(atropine should
always be given before)-
Laryngeal spasm may occur
Post operative nausea and
vomiting frequent
Recovery slow
Cause hyperglycemia-
contraindicated in diabetic pt.
Not preferred now
20.
Halothane
Colorless liquidwith sweet odor, Non irritant and non-inflammable
Store in dark bottle to prevent decomposition by light(thymol added
as preservatives)
Advantages Disadvantage
Potent non inflammable,
Non irritant anesthetic
Smooth and rapid
induction of anaesthesia
with rapid recovery
Low incidence of nausea
and vomiting
Cause-
bronchodilatation-
preferred in asthma
Poor analgesic among inhalational agents
& poor muscle relaxant
CVS:-Hypotension: It has direct
depressant effect on the myocardium and
causes hypotension
Contraindicated-labour(uterine relaxant)
Cause-Malignant Hyperthermia-Rx
dantrolene
Post anaesthetic chill, shivering-Rx-
pethidine
Hepatotoxicity
21.
Isoflurane
• Non-inflammable andnon-explosive, colourless volatile
liquid
• No liver toxicity & does not provoke seizures
• Hypotension-↓PvR-use in cardiac surgery
• Preferred in neurosurgical procedures-milder cerebral
vasodilatation
• Routinely used for maintenance anesthesia
• Use in Neuro-surgical anaesthesia- due to ↓cerebral
metabolic rate & ↓02 consumption of brain also doesn’t
↑ICT
• Expensive
• Coronary steal phenomenon
22.
Desflurane
• Congener ofisoflurane
• Low blood and tissue solubility
• Fast inducing agents-suitable for day care surgery
• recovery rapid and smooth
• Preferred for old age, long surgeries, renal & hepatic
pt.
• Special apparatus is required-vaporizer(boil at room
temp.)
• Transient sympathetic stimulation
• Good alternative to isoflurane
23.
Savoflurane
• Newer inhalationalagent
• No pungent smell
• Rapid and smooth induction(2 min)
• Good muscle relaxation with poor Analgesia
• Does not produce coronary steal phenomenon
• Good choice in children-rapid & smooth induction
• Disadvantages:-
• May precipitate malignant hyperthermia
24.
Intravenous Anesthetics
• Thisare drug that when given intravenously in a
appropriate dose cause rapid loss of consciousness
Single I.V. bolus I.V. infusion
Rapidly redistributed to
skeletal muscle and skin
A bolus is ideal for
induction, short
procedures and as a
supplement
To maintain the
anaesthesia for long
procedure
Agents that are rapidly
metabolized
25.
Thiopentone sodium:-
• Ultrashort acting barbiturate
• Commonly used i.v. anaesthetic for induction of anaesthesia
• Hypnosis and anesthesia without analgesia
• Highly alkaline (pH 10.5–11), hence highly irritant-Should
not be mixed with acidic drugs
• Extravasations-pain, necrosis and gangrene
• Duration:6-10 minutes
• Highly lipid soluble, crosses BBB and undergoes
redistribution-rapid onset & short duration(5-8min)
• Cause hypotension-venodilatation, direct myocardial
depression
• Eye-↓IOP
26.
Side effect:-
Local:-I.m. injection-ulceration-local necrosis
Intra-arterial injection:-Due to alkaline nature-precipitate in arterial
pH-leading to gangrene
General-
o Respiratory depression, Cardiovascular depression
o Hiccups, Laryngeal spasm
o Coughing,Dysphonia, delirium
Uses
1. Thiopentone sodium is used for induction of anaesthesia.
2. It is occasionally used as anticonvulsant in cases not controlled by
other drugs
Contraindicated-acute intermittent porphyria-It can precipitate
27.
Propofol
• Most commonlyuse inducing agent for out-patient surgical procedure
• Propofol:1-2% emulsion in soyabean oil-so injection is painful (given
along with 1% xylocaine)
Advantage Disadvantage
o Quick induction-15-30 esc. Last
for 5-8 min
o Smooth, pleasant, low incidence
of voluntary movements
o Recovery rapid & smooth than
thiopentone
o Has superseded thiopentone
o Processed-Cerebroprotective,
Anti-emetic, Anti-pruritic action
o Safe in pregnancy
o Use as-iv bolus As well as
o No analgesic or muscle relaxant
property
o Apnoea more common & longer
than thiopentone
o Hypotenison- is significant
o Pain-site of bolus injection
28.
Use:-
I.V. propofolis useful for the induction of anaesthesia in
adults
Anaesthesia of choice for Day care surgery
I.V anaesthetic of choice in ICU- Frequently used to sedate
intubated patients
I.V anaesthetic of choice in malignant hyperthermia
Resistance case of Status epilepticus
Fospropofol:-
Water soluble prodrug of propofol
Slower onset & lack of side effect of propofol
29.
Etomidate
• Duration: 5-10minutes
• Less CVS & Resp depression
• Disadvantages:
• Pain on injection, Excitatory muscle movements,
nausea and vomiting, poor analgesic, HPA axis
supression
• Occasionally used as emergency anesthesia-less
hypotension
30.
Ketamine-Dissociative anesthesia
• “Dissociativeanesthesia”-pt. feels dissociated from the surrounding
as well from own body due to inhibition of cortical function &
thalamus leading to stimulation of limbic system
• Associated characteristics- Amnesia, Analgesia, sedation,
unresponsiveness to commands
MOA:- no action on ARAS. Blocks action of glutamate at NMDA
receptor
• It is commonly given by i.v. route; other routes are i.m., oral and
rectal
Advantage:-
↑ HR, ↑ CO, ↑ BP, ↑PR- i.v. anesthetic of choice-hypovolemic Shock
pt.
Impairment of pharyngeal & laryngeal reflex-good for full stomach pt
Bronchodilatation-sympathetic stimulation-suitable for asthma pt.
31.
Disadvantage:-
Slow onsetof action
No-muscle relation action
↑ Cerebral blood flow and ↑ICT-contraindicated in head injury
Produce-Hallucination, disorientation
Contraindicated-hypertension, MI, pregnancy (uterine contraction)
USE:-
Minor surgeries
Safe anaesthetic to be used as remote place & inexperience hand(since
no Respiratory depression)
I.V. anaesthetic choice for shock pt
Can be use in asthmatic pt
Preferred agent when pt is full stomach
Due to analgesic properties-good for burn dressing
Pt who lost circulatory volume due to dehydration, haemorrhage &
shock (Road side accident)-where GA cant be given
32.
Opioids
• Opioids usein anaesthesia- fentanyl, alfentanil, sufentanil,
remifentanil and pethidine
• Potent analgesics
• can be used along with anaesthetics—↓requirement of
anaesthetic
• Sulfentanil-most potent
• Alfentanil-use in Day care surgery
• Shortest acting- remifentanil-due to rapid metabolism by
esterase-preferred-hepatic disease pt.
33.
Drug useful forday care surgery
• Desflurane
• Midazolam(BZD)
• Sevoflurane
• Alfentanil
• Propofol
• Mivacurium
34.
Conscious Sedation
• Conscioussedation is a level of CNS depression where a patient
does not lose consciousness but is able to communicate and
cooperate during the procedure/treatment
State of altered consciousness
Indications:-
• Uncooperative patients.
• Anxious patients.
• Emotionally compromised patients.
Conscious sedation should be avoided in:-
• Chronic obstructive pulmonary disease.
• Pregnancy.
• Prolonged surgery.
• Psychoses.
Preanesthetic Medication(PAM)
• Objectives:
1.Relief of anxiety and apprehension
2. ↓ secretions and vagal stimulation
3. Supplement analgesic action GA and potentiate
them
4. To induce amnesia
5. Reduce chances of emesis
It is the use of drugs before the administration of
anaesthetics to make anaesthesia more pleasant and safe.
1.To reduce anxietyand apprehension:-
Preferred drug-Benzodiazepines like diazepam, lorazepam or
midazolam
Advantage-
sedative, amnesic, calming, anxiolytic effects and wide margin of
safety.
↓anxiety by acting on limbic system
Chlorpromazine-as neuroleptics-sedation+Anti-emetics
2. To prevent vagal bradycardia and reduce salivary secretions
caused by anaesthetics:-
• Atropine/glycopyrrolate(preferred-less CNS Side effect, long acting) –
Advantage:-
↓salivary and bronchial secretions(prevent laryngospasm ).
Prevent vagal bradycardia and hypotension.
Hyoscine-produce sedation, amnesia, Antiemetic
39.
3.To relieve pre-and post-operative pain:-
Opioid analgesics such as morphine, pethidine or fentanyl
Advantage:-
Relieve pre & post-op pain
Sedation & Anxiolytic action
Reduction in dose of GA
NSAIDs like diclofenac can also be used.
4. For antiemetic effect:-
Drug-Metoclopramide, domperidone or ondansetron (to
control vomiting)
Advantage:-
-prevent Post-op vomiting
-prevent Aspiration pneumonia
40.
5. To preventacid secretion and stress ulcer:-
H2-Blocker -ranitidine
proton-pump inhibitor(PPI)-omeprazole – (↓reduce gastric
acid secretion especially before prolonged surgery)
Antacides-neutralized the gastric acidity
6.To hasten gastric emptying before emergency surgery:-
Drug-Metoclopramide or domperidone-prokinetic agents
Advantages:-
↑tone of lower esophageal sphincter
accelerate gastric emptying, thus prevent aspiration
pneumonia.
41.
Complications of GA
•Hypoxia
• Nausea, vomiting
• Dislocation of temporomandibular joint
• Persisting sedation
• Cardiac arrhythmias, especially with halothane
• Subcutaneous emphysema of face can occur rarely
• Hyperthermia
42.
Question paper discussion:-
Q.Write a short note on:- Propofol (4M) 14,17
Q. Write a short note on:-Ketamine (2.5M) 12,10
Q.
Classify general Anaesthetic agents. Giving suitable example. Discuss
the importance of preanesthetic medication (4+4=8)