• Sedative:-Drug thatreduces excitement and produces
calmness of the mind without inducing sleep.
• Hypnotic:-drug that produces sleep resembling normal
sleep.
• Sleep-A state of unconsciousness but still able to awaken
by normal sensory stimuli
• Type-NREM & REM sleep
• Sleeping between 7-9hr per night appears to be optimal for
health in adults aged ≥18 years
3.
• Sleeping <7h is associated with adverse outcomes,
• Obesity
• Diabetes,
• Elevated blood pressure,
• cardiovascular depression,
• All-cause mortality,
• Physiological disturbances such as impaired immune
function
• increased pain sensitivity
• impaired cognitive performance
4.
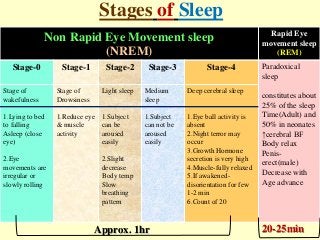
Stages of Sleep
NonRapid Eye Movement sleep
(NREM)
Rapid Eye
movement sleep
(REM)
Stage-0 Stage-1 Stage-2 Stage-3 Stage-4 Paradoxical
sleep
constitutes about
25% of the sleep
Time(Adult) and
50% in neonates
↑cerebral BF
Body relax
Penis-
erect(male)
Decrease with
Age advance
Stage of
wakefulness
1.Lying to bed
to falling
Asleep (close
eye)
2.Eye
movements are
irregular or
slowly rolling
Stage of
Drowsiness
1.Reduce eye
& muscle
activity
Light sleep
1.Subject
can be
aroused
easily
2.Slight
decrease
Body temp
Slow
breathing
pattern
Medium
sleep
1.Subject
can not be
aroused
easily
Deep cerebral sleep
1.Eye ball activity is
absent
2.Night terror may
occur
3.Growth Hormone
secretion is very high
4.Muscle-fully relaxed
5.If awakened-
disorientation for few
1-2 min
6.Count of 20
Approx. 1hr 20-25min
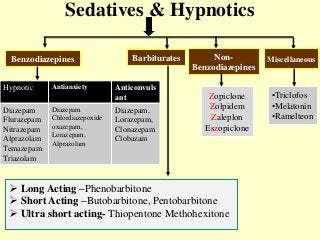
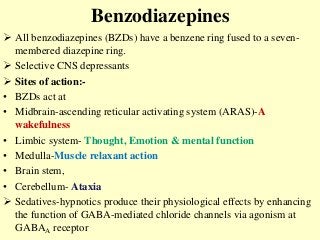
Benzodiazepines
All benzodiazepines(BZDs) have a benzene ring fused to a seven-
membered diazepine ring.
Selective CNS depressants
Sites of action:-
• BZDs act at
• Midbrain-ascending reticular activating system (ARAS)-A
wakefulness
• Limbic system- Thought, Emotion & mental function
• Medulla-Muscle relaxant action
• Brain stem,
• Cerebellum- Ataxia
Sedatives-hypnotics produce their physiological effects by enhancing
the function of GABA-mediated chloride channels via agonism at
GABAA receptor
7.
GABAA Receptor
Cl-
Cl
GABAA receptor is a pentameric structure
Compose of varying polypeptide subunit associated with a chloride
channel on the postsynaptic membrane
8.
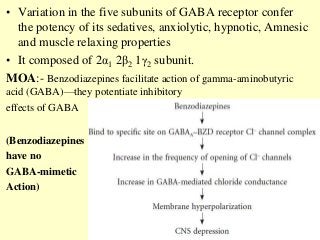
• Variation inthe five subunits of GABA receptor confer
the potency of its sedatives, anxiolytic, hypnotic, Amnesic
and muscle relaxing properties
• It composed of 2α1 2β2 1γ2 subunit.
MOA:- Benzodiazepines facilitate action of gamma-aminobutyric
acid (GABA)—they potentiate inhibitory
effects of GABA
(Benzodiazepines
have no
GABA-mimetic
Action)
9.
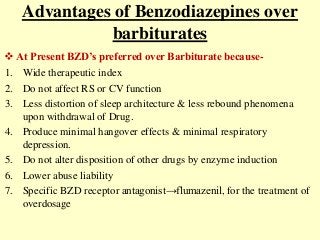
Advantages of Benzodiazepinesover
barbiturates
1. Wide therapeutic index
2. Do not affect RS or CV function
3. Less distortion of sleep architecture & less rebound phenomena
upon withdrawal of Drug.
4. Produce minimal hangover effects & minimal respiratory
depression.
5. Do not alter disposition of other drugs by enzyme induction
6. Lower abuse liability
7. Specific BZD receptor antagonist→flumazenil, for the treatment of
overdosage
At Present BZD’s preferred over Barbiturate because-
Pharmacokinetics
• Absorption:- Rapid& complete orally
• Administered-orally or intravenously occasionally by rectal route
(diazepam) in children
• IM absorption is irregular (except for lorazepam)
• Distribution-
Lipophilic, cross BBB
Large volume of distribution
Can cross placental barrier also
• Metabolism:- liver by hepatic microsomal enzymes(CYP3A4) except
lorazepam, oxazepam, temazepam so this can be given in hepatic
failure & elderly pt.
• Some of them produce active metabolites that have long half-life e.g.
flurazepam
• Excretion:- Urine
12.
-:Pharmacological Action:-
1.CNS:- (Sedation& hypnosis)
Low dose-Drowsiness ,sedation
Dose increases-hypnotics
Sleep induced-not natural (due to ↓REM sleep)
Withdrawal drug-cause rebound ↑REM sleep
↓sleep latency-shorten the time to fall asleep
↑ total sleep time & ↓intermittent night awakening
Long term use-develop tolerance (thus dose has to be ↑↑)
Anterograde amnesia
Anxiolytic action:- (due to action on limbic system)
occurs in dose lower than hypnotics dose
No development of tolerance-in anxiolytic dose
13.
Anticonvulsant action-(↑Seizure threshold)
Potent Anticonvulsant-effective in all types of epilepsy but
tolerance develops upon chronic use.
Central muscle relaxant action-
↓Muscle tone-
↓muscle spasm-
• Respiratory system:-
– at hypnotic and lower doses, no significant effect
– at higher doses, may promote apnea(Respiratory
depressant)
( ) polysynaptic reflex in spinal cord
14.
• Cardiovascular system
–therapeutic doses-No significance change
– High dose/iv administration hypotension
• Gastrointestinal tract
– Prevent stress ulcers by ↓Nocturnal gastric secretion
– No significant effect-bowel movement
15.
-:Therapeutic Uses:-
1.Insomnia:- Ashypnotic
It’s a symptom-if persistently for more than 3-4 night
Symptoms include-
(1.) Not able to fall asleep within-30-45min
(2.) more than 5-6 awakening/night
(3.) less than 6hr of sleep in normal adult
Cause:-
Social/personal problems-illiness, unemployment, family problems
Psychiatric disorder-Schizophrenia, depressant, Anxiety
Other disease-Asthma,CHF,Migraine & pain,headache
Drug & food-ephedrine,Amphetamine,coffee,tea,nicotine,
Types of insomnia:-
Transient insomnia (less than 3 days)- cause –environmental or
16.
• Also canoccur due to Shift work, overnight work, change
in work pattern/new place, Jet lag
℞- Zolpidem (5/10mg HS), Zaleplon (Z-compound)/short
acting BZD’s like triazolam(0.5mg)
• Short term insomnia (3days-3 weeks)- cause due to
social/personal problem(unemployment, job problem,
family problem)
℞-Zopiclone, Eszopiclone (half an hour before going to bed in
lowest dose)
Withdrawal of drug should be gradual to prevent rebound
insomnia
• Long term insomnia (more than 3 weeks):- Non-
pharmacological therapy like exercise, sleep hygiene
17.
Non-Pharmacological Treatment
Educationabout sleep hygiene
Room ventilation
Avoids-CNS stimulants like caffeine,tobacco
Warm sweet Milk intake-d-tryptophan ↓time of onset of
sleep
Elderly should restrict-fluid intake in the evening to
reduced nocturia
Avoid day time napping
Morning physical exercise-yoga, Meditation
Sleep restriction therapy-sleep 30-60min less than usual
duration which help in onset of sleep
18.
2.Anxiety:- due toanxiolytic action.
longer acting drug like Alprazolam, lorazepam, oxazepam,
diazepam preferred
Clonazepam-panic disorder. The anxiolytic effect is due to their
action on limbic system
3. Epilepsy:- due to anti-convulsant action
Absence seizure-clonazepam, clobazam
Status epilepticus-lorazepam, diazepam(as they enter brain)
4.Skeletal Muscle spasm:- (Centrally acting)
Acute muscle spasm
Spinal injury-inhibit polysynaptic reflex
5. Preanesthetic medication:- (due to its sedative–amnesic and
anxiolytic effects) Hence, the patient cannot recall the perioperative
events later- lorazepam, midazolam
GA- I.V. Diazepam, lorazepam, midazolam, + other central nervous
system (CNS) depressants
Side Effects andToxicities
Common side effects-
Drowsiness, confusion, blurred vision, amnesia, disorientation
Tolerance- to sedative-hypnotic effect(less than barbiturate)
Dependence (physical& psychological)-least physical dependance
More common with Diazepam, Alprazolam
Withdrawal after chronic use:-
Tremor, insomnia, restlessness, nervousness and loss of
appetite.
Use of BZDs during labour-
respiratory depression and hypotonia, hypothermia in the new-born
21.
Interaction
1. BZD’s ×Alcohol- potentiate CNS depressant
action
2. BZD’s × Anti-histaminics, opioids (other CNS
depressant) potentiate CNS depressant action of
BZD’s
3. BZD’s × CYP3A4 inhibitors (Erythromycin,
Ketoconazole)- inhibit metabolism of BZD’s leading to
prolong the action
4. BZD’s ×Valproate-psychotic attack
22.
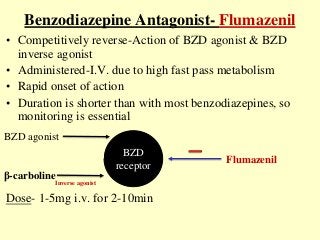
Benzodiazepine Antagonist- Flumazenil
•Competitively reverse-Action of BZD agonist & BZD
inverse agonist
• Administered-I.V. due to high fast pass metabolism
• Rapid onset of action
• Duration is shorter than with most benzodiazepines, so
monitoring is essential
Dose- 1-5mg i.v. for 2-10min
BZD
receptor
BZD agonist
β-carboline
Inverse agonist
Flumazenil
23.
• Withdrawal (agitation,tremors seizures) may be
induced in patients who either abuse or chronically
take benzodiazepines for therapy
• Used:-
• overdose of benzodiazepines to reverse sedation &
respiratory depression
• To reverse Sedative effect of BZD’s(higher dose)
during general anesthesia
• Reverse the hypnotics effect of Z-compounds
SE:- confusion, dizziness and nausea.
24.
Non-Benzodiazepine Hypnotics
Alsocalled as “Z” compounds-name started with Z
Less abuse potential than BZD’s & short duration of action
Less effect on REM sleep than BZD’s-negligible disruption
of sleep architecture
Over dose can be antagonized by flumazenil
They are preferred over BZD’s-
Sedative & hypnotic action equal with BZD’s
Wide margin of safety-safe long use (up to 12 month)
Week anxiolytic action
No anti-convulsant & central muscle relaxant action
No amnesia occurs
25.
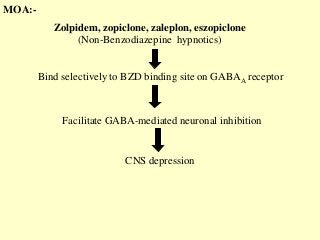
Zolpidem, zopiclone, zaleplon,eszopiclone
(Non-Benzodiazepine hypnotics)
Bind selectively to BZD binding site on GABAA receptor
Facilitate GABA-mediated neuronal inhibition
CNS depression
MOA:-
26.
Zolpidem:-
• Chemically unrelatedto benzodiazepines or barbiturates-
imidazopyridine group of drug
• Rapidly acting within 15 minutes of oral dose
• Mainly produce hypnosis, but no muscle relaxant or
anticonvulsant effects
• No effect on REM sleep
• T1/2-2hr
• ↓sleep latency ↑duration of sleep time
• Minimal hangover effect & rebound insomnia
• Less likely to cause tolerance & dependance
• Used for transient insomnia/short term insomnia
• SE- headache, confusion, Nausea, vomiting
27.
Zopiclone-newer agent
• Effecton sleep resemble that of BZD
• Do not prolong REM sleep
• Prolongs Stage 3 & 4
• Does not disturb sleep architecture or hangover or
withdrawal
• T1/2-5hr
• Use:- Short term insomnia
• Side effects:-
• Metallic taste, impaired judgment (liable to road
traffic accident), dry mouth
28.
Zaleplon
• Used insleep onset insomnia
• Absorbed orally & rapidly-shortest acting “z”
compound
• Sustained efficacy on prolong use
• T1/2-1hr
• Preferred in bed time
• Bioavailability 30%-extensive first pass metabolism
• Safest among other drugs
29.
Eszopiclone
• Enantiomer ofzopiclone
• Reduced sleep latency
• No after use of drug on next day
• No tolerance reported
• Used in short insomnia
• Effect blocked by Flumazenil
30.
Barbiturates
• Derivatives ofbarbituric acid-Acidic drug
• Used Earlier-upto 1960-not used now
• High incidence of
accidental,
suicidal, and
homicidal attempts and completions
• Non-selective CNS depressant
• Site of Action-ARAS main site of action
Duration of action is very important clinically-
Long acting barbiturate-used as anti-epileptics
Short acting barbiturate-sedative-hypnotics & anxiolytics
Ultra-shorting barbiturate-used for anesthetic induction
31.
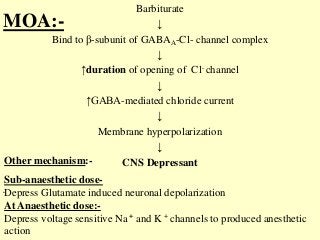
MOA:-
Barbiturate
↓
Bind to β-subunitof GABAA-Cl- channel complex
↓
↑duration of opening of Cl- channel
↓
↑GABA-mediated chloride current
↓
Membrane hyperpolarization
↓
CNS Depressant
•
Sub-anaesthetic dose-
Depress Glutamate induced neuronal depolarization
At Anaesthetic dose:-
Depress voltage sensitive Na + and K + channels to produced anesthetic
action
Other mechanism:-
-:Pharmacokinetics:-
Absorption- orally rapid,Food delay absorption
Distribution-widely in body
High lipid soluble-higher potency
Thiopentone sodium processed-redistribution
Barbiturate-acidic in nature
Metabolism:- liver by glucuronide conjugation &
oxidation
Excretion:- urine
34.
Pharmacological Action
1.CNS:- CNSdepressant
Sedatives & hypnotics:-
Low dose-sedation
Hypnotic dose-↓sleep latency and night awakenings,
↑duration of sleep
At present, barbiturates are not recommended because:
They have a low therapeutic index.
They cause rebound increase in REM sleep on stoppage of therapy(nightmares
).
They cause marked respiratory depression.
They produce marked hangover effects (headache and drowsiness on waking).
They cause high degree of tolerance and drug dependence.
They are potent enzyme inducers and cause many drug interactions.
They have no specific antidote.
35.
Anti-convulsant effect:- Phenobarbitone
Tolerancedoesn’t develop to anti-convulsant dose
General anaesthetic effect:- capable of producing surgical
anaesthesia
Can impair learning, memory & judgment
Depress all areas of CNS, Maximum-reticular activating
system
Respiratory system-Dose dependent depression (hypnotic
dose/higher dose)
CVS-Overdose produce marked hypotension(hypnotic dose
& anesthetic dose) due to ↓COP & Venous return
Toxic dose-suppression to VMC-cardiac arrest
Kidney:- ↓urine volume(oliguria)-poor urine formation
Side Effects:-
1. CommonSide Effect-
Drowsiness, confusion, headache, ataxia, hypotension and
Respiratory depression.
2. Hypersensitivity reactions like skin rashes, itching and
swelling of face may occur.
3. Tolerance develops to their sedative and hypnotic actions on
repeated use.
4. Physical and psychological dependence develops on
repeated use.
5. Phenobarbitone Prolonged use - megaloblastic anemia by
interfering with absorption of folic acid from the gut.
38.
• 6. Precipitateattacks of acute intermittent porphyria-
barbiturate-increase δ-aminolevulenic acid
synthetase(D-ALA)-rate limiting enzyme in
Porphyrin synthesis- leading to accumulation of
toxic porphyrin precursors in the body
• 7. In case of acute barbiturate poisoning, the signs
and symptoms are drowsiness, restlessness,
hallucinations, hypotension, respiratory depression,
convulsions, coma and death.
39.
Acute barbiturate poisoning
Suicidal or rarely accidental
Short-acting preparation are more lethal at lower dose
Fatal dose-lipid soluble drug-2-3 gm , less lipid soluble
phenobarbitone- 6-10 gm
Symptoms:-
o Metabolic coma
o Sever respiratory & cardiovascular depressant
o Acute renal failure
o Pulmonary edema
o Barbiturate blisters-due to deposition
Of porphyrin
Uses
A. For inductionof anesthesia & short surgical
procedure:- Thiopentone sodium-i.v.
B. Antiepileptic- phenobarbitone
status epilepticus in children
Eclampsia
Young children with recurrent febrile seizures
C. Neonatal jaundice & kernicterus
Contraindication
Acute intermittent porphyria-barbiturate↑ δ-
aminolevulenic acid synthetase-rate limiting
enzyme in porphyrin synthesis-leading to
accumulation of toxic porphyrin precursors in the
body
Liver & kidney disease
Sever pulmonary insufficiency
44.
Melatonin
Naturally occurringparacrine hormone of pineal glad in
brain
“Hormone of darkness”-secrete at night & maintained
the body circadian rhythm
Acts via Melatonin recptor-MT1 & MT2-(GPCR) found in
membranes of neurons of suprachiasmatic nucleus of
hypothalamus
Melatonin process-
Anti-oxidant,
immunostimulant action,
anti-cancer,
maintained BP during sleep.
45.
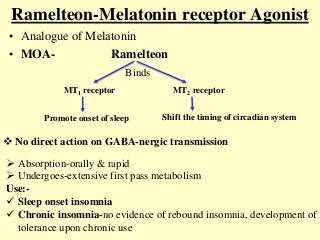
Ramelteon-Melatonin receptor Agonist
•Analogue of Melatonin
• MOA- Ramelteon
Binds
MT1 receptor MT2 receptor
Promote onset of sleep Shift the timing of circadian system
No direct action on GABA-nergic transmission
Absorption-orally & rapid
Undergoes-extensive first pass metabolism
Use:-
Sleep onset insomnia
Chronic insomnia-no evidence of rebound insomnia, development of
tolerance upon chronic use
46.
Questions
Q. Write shortnote on:
1.Non-Benzodiazepine hypnotics/Z compounds
2.Benzodiazepines
Q. Discuss the pharmacological basis for the use of
• Benzodiazepines are preferred over barbiturate in the
treatment of insomnia
• Barbiturates are contraindicated in Acute intermittent
porphyria
Q. Write mechanism of action, uses & adverse effect of
diazepam
Q. Pharmacotherapy of Insomnia
Editor's Notes
#5 Night terror-Episodes of screaming, intense fear and flailing while still asleep
Dreaming sleep-paradoxical sleep
One sleep cycle-1hrNREM+REM-total 4-5 sleep cycle every night
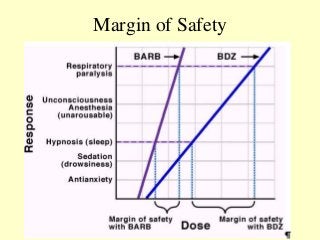
#11 Barbiturate steeper DRC process narrow margin of safety
#12 Rectally diazepam-use in febrile seizure (fever induced seizure)
#13 Pt cant recall the perioperative event due to amnesia action-so that can be used as Preanesthetic medication
Anterograde amnesia –pt unable to form new memories
#16 Adults-1-2 awakening per night considered normal
#17 Long-term use of BZDs for insomnia is not recommended because of tolerance, dependence and hangover effects
Zolfresh-5mg HS-Zolpidem
Valium 2/5/10-diazepam
#29 Can be taken by pt. who is awake In the middle of night & not able to sleep
#37 Kernicterus-a type of brain damage that can result from high levels of bilirubin in a baby's blood
cerebral palsy and hearing loss. Kernicterus also causes problems with vision and teeth and sometimes can cause intellectual disabilities
#39 acute intermittent porphyria-abdominal pain, difficulty in micturition,parasthesia
It can be precipitated by-Ocps,sulfar containg drugs





















![Parkinson's Disease [Advanced Pharmacology]](https://cdn.slidesharecdn.com/ss_thumbnails/07-210419085948-thumbnail.jpg?width=640&height=640&fit=bounds)



























