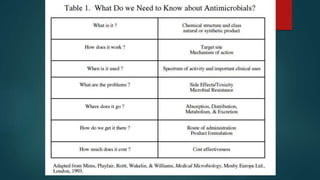
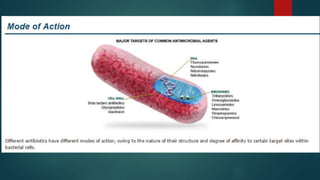
This document discusses various classes of antimicrobial agents used to treat bacterial, viral, and fungal infections. It describes the mechanisms of action and examples of drugs that inhibit cell wall synthesis, cell membrane function, protein synthesis, nucleic acid synthesis, and other metabolic processes in bacteria. It also discusses mechanisms of drug resistance in bacteria and summarizes treatment approaches for herpes virus infections and HIV/AIDS.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















