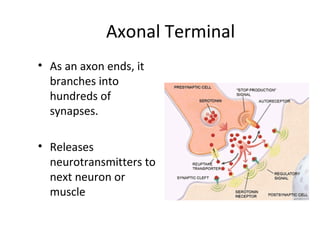
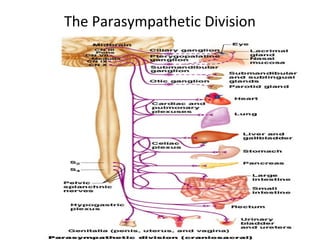
The nervous system has two main divisions: the central nervous system (CNS) and the peripheral nervous system (PNS). The autonomic nervous system (ANS) is a division of the PNS and controls involuntary body functions. It has two branches - the sympathetic and parasympathetic systems. The sympathetic system activates the fight or flight response while the parasympathetic system activates the rest and digest response. Both systems involve a two-neuron chain with a preganglionic neuron originating in the CNS and a postganglionic neuron that releases neurotransmitters like acetylcholine and norepinephrine.































































































![Subdivisions of the Autonomic Nervous System
Sympathetic Parasympathetic
Primary
Neurotransmitter
norepinephrine
epinephrine (~20%)
acetylcholine
Receptors
&
Second
Messenger
Systems
Adrenergic GPCRs
α1 – IP3/DAG, ↑[Ca2+
]i ↑PKC
α2 - ↓cAMP/PKA
β1 - ↑cAMP/PKA
β2 - ↑cAMP/PKA
β3 - ↑cAMP/PKA
Muscarinic GPCRs
M1 – IP3/DAG, ↑[Ca2+
]i ↑PKC
M2 – ↓cAMP/PKA, ↑PI(3)K
M3 – ↓cAMP/PKA,
IP3/DAG, ↑[Ca2+
]i ↑PKC
M4 –
M5 – IP3/DAG, ↑[Ca2+
]i ↑PKC
Adrenal Medulla
(epi:norepi::80:20)](https://image.slidesharecdn.com/anscns-160607205009/85/ANS-SYMPATHETIC-and-PARASYMPATHETIC-107-320.jpg)















![OH OP
[2]
degradation
to VMA
insulin activation of protein
phosphatase to dephosphorylate
enzymes[7]
α
[5]
γ
β
GTPase
αGDP
epinephrine
phosphorylation
of β-receptor by
β-ARK decreases
activity even with
bound hormone
OH OH
[3]
OP OP
[4]
OPOP
binding of β-arrestin
further inactivates
receptor despite
bound hormone
AC
cAMPATP
activated PKA
phosphorylates
enzymes
[6]
AMP
phosphodiesterase
GTP
[1]
dissociation
Figure 6. Mechanisms for terminating the signal generated by epinephrine
binding to a β-adrenergic receptor](https://image.slidesharecdn.com/anscns-160607205009/85/ANS-SYMPATHETIC-and-PARASYMPATHETIC-123-320.jpg)