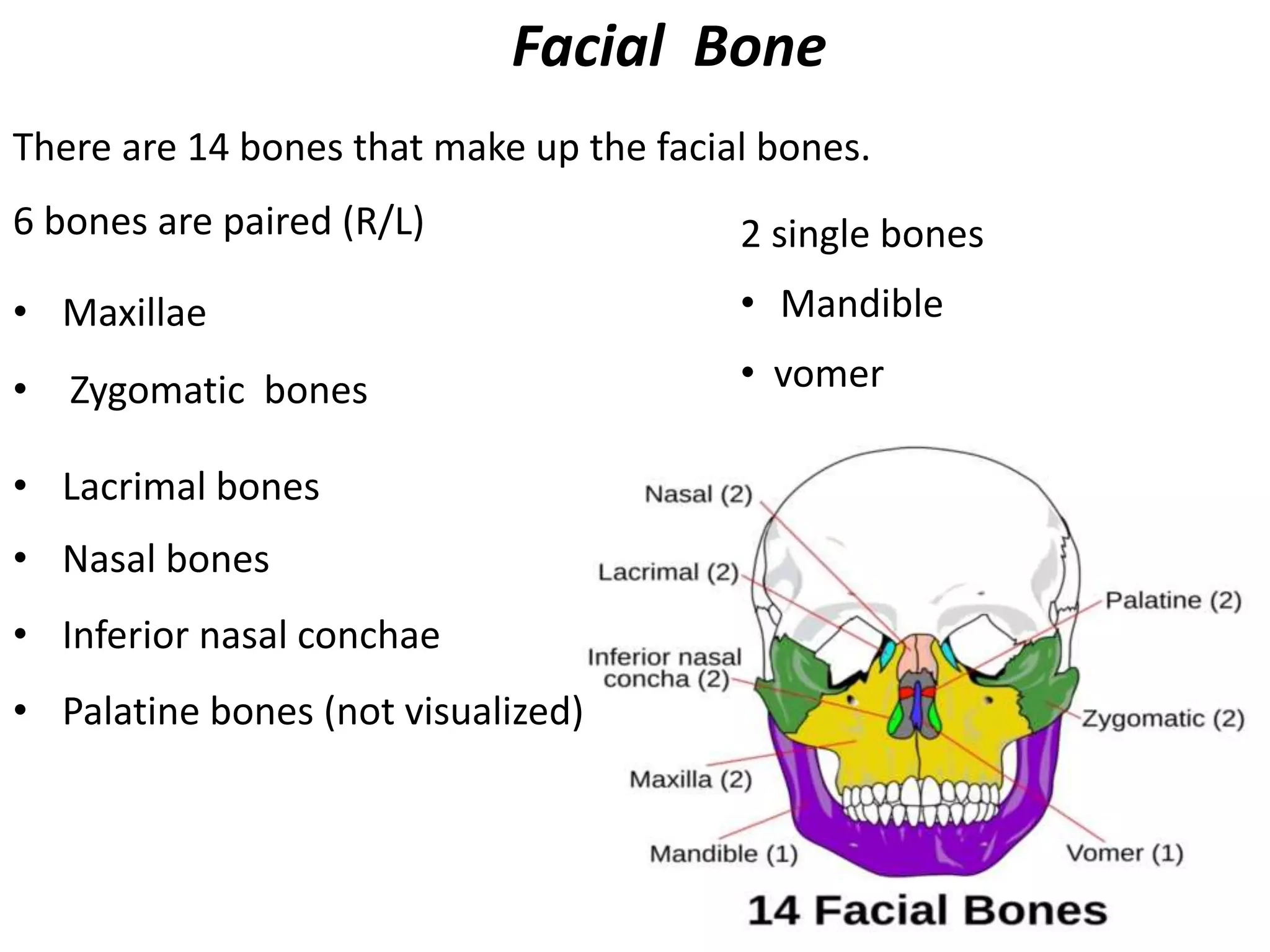
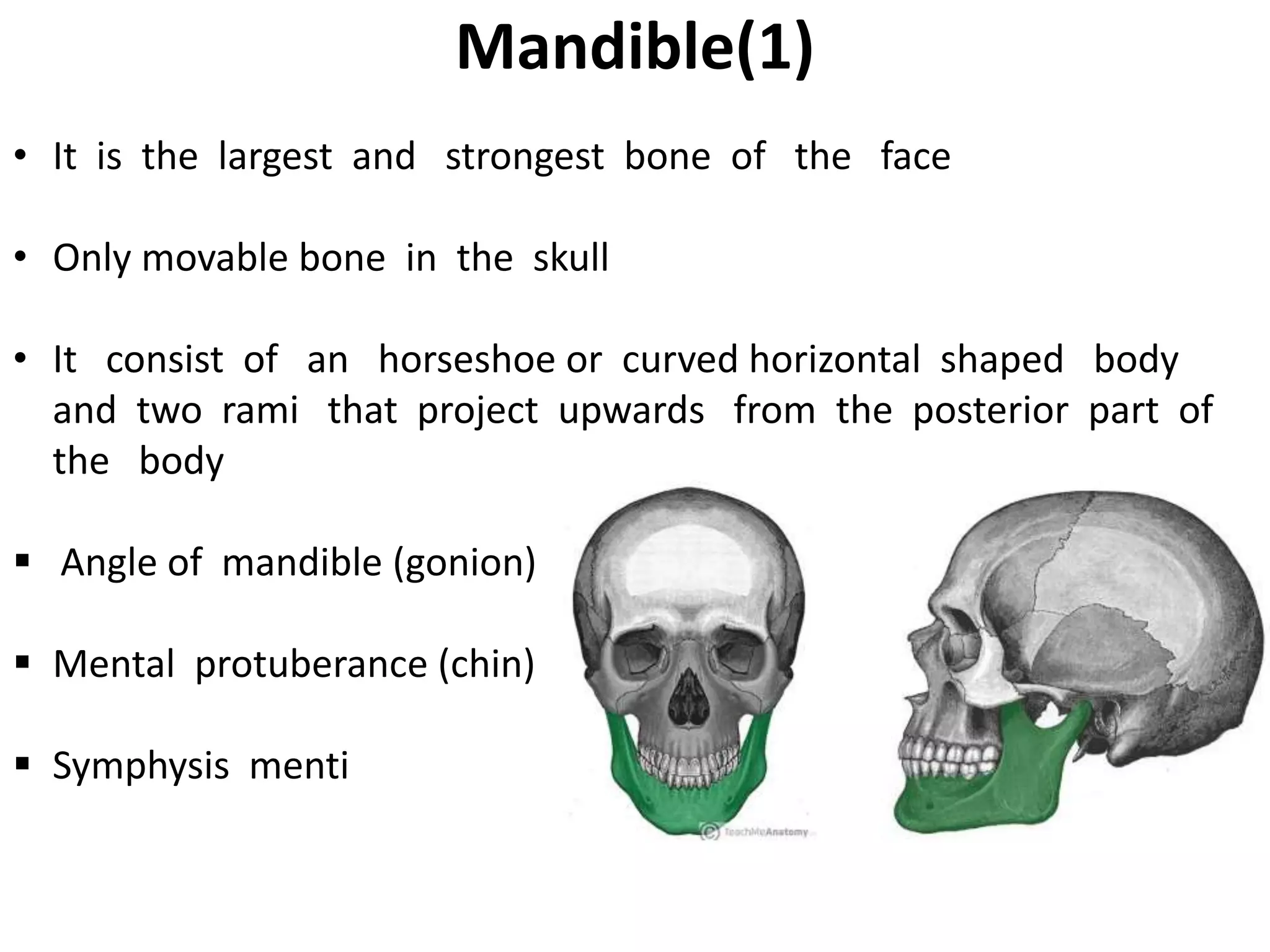
1) The document provides an overview of facial bone anatomy and radiographic interpretation of facial bone radiographs. It describes the 14 facial bones and their key features and relationships.
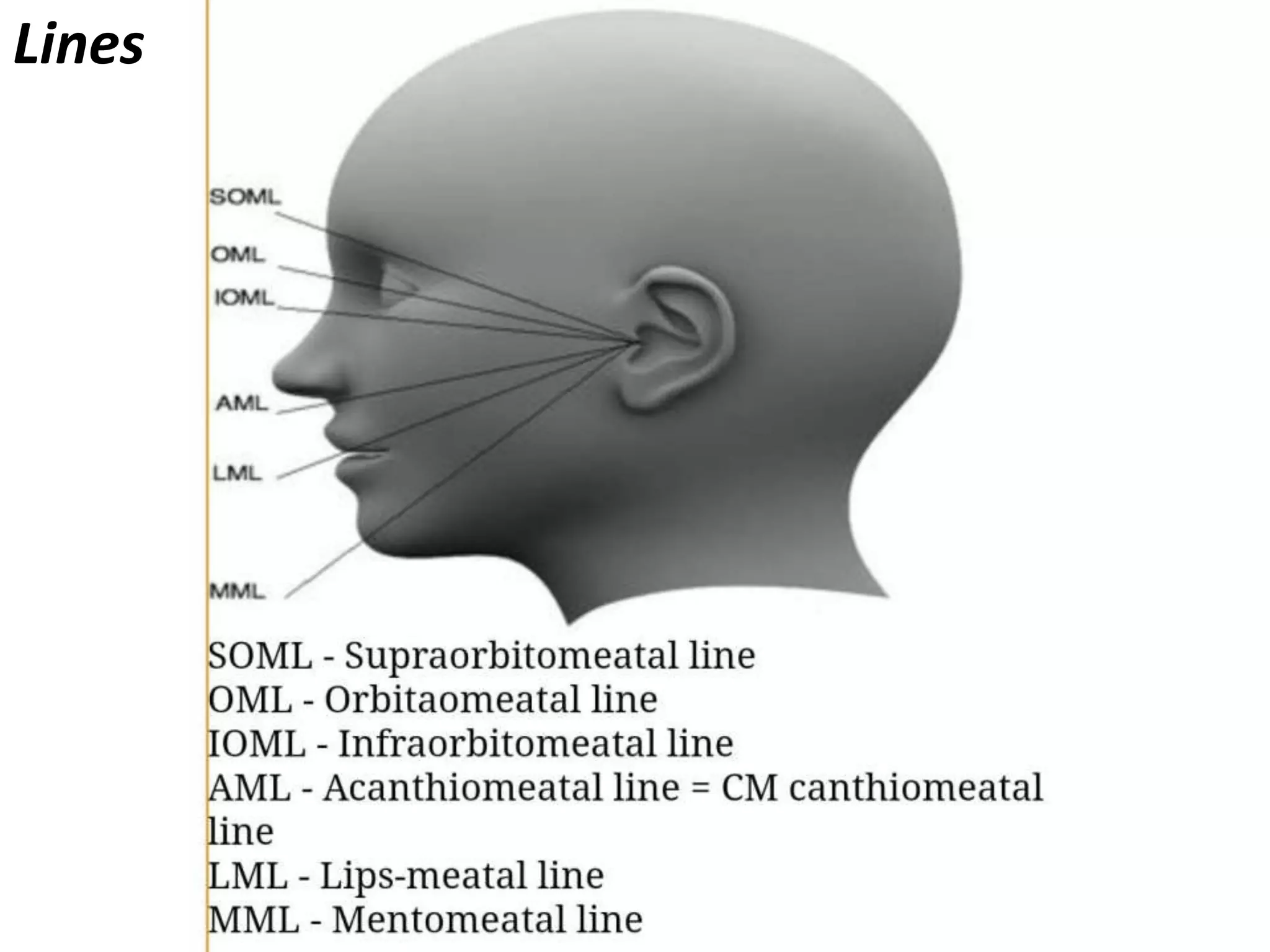
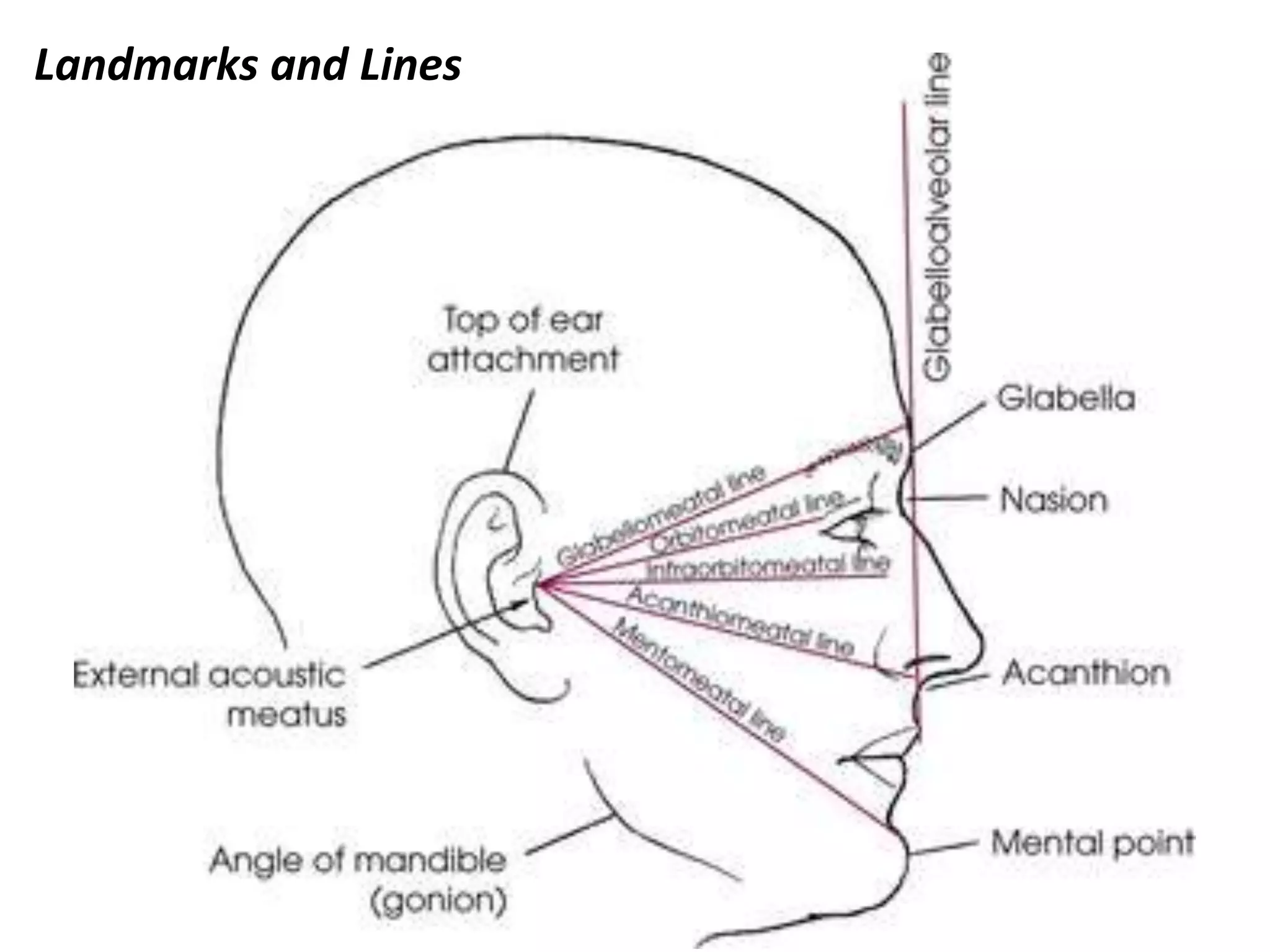
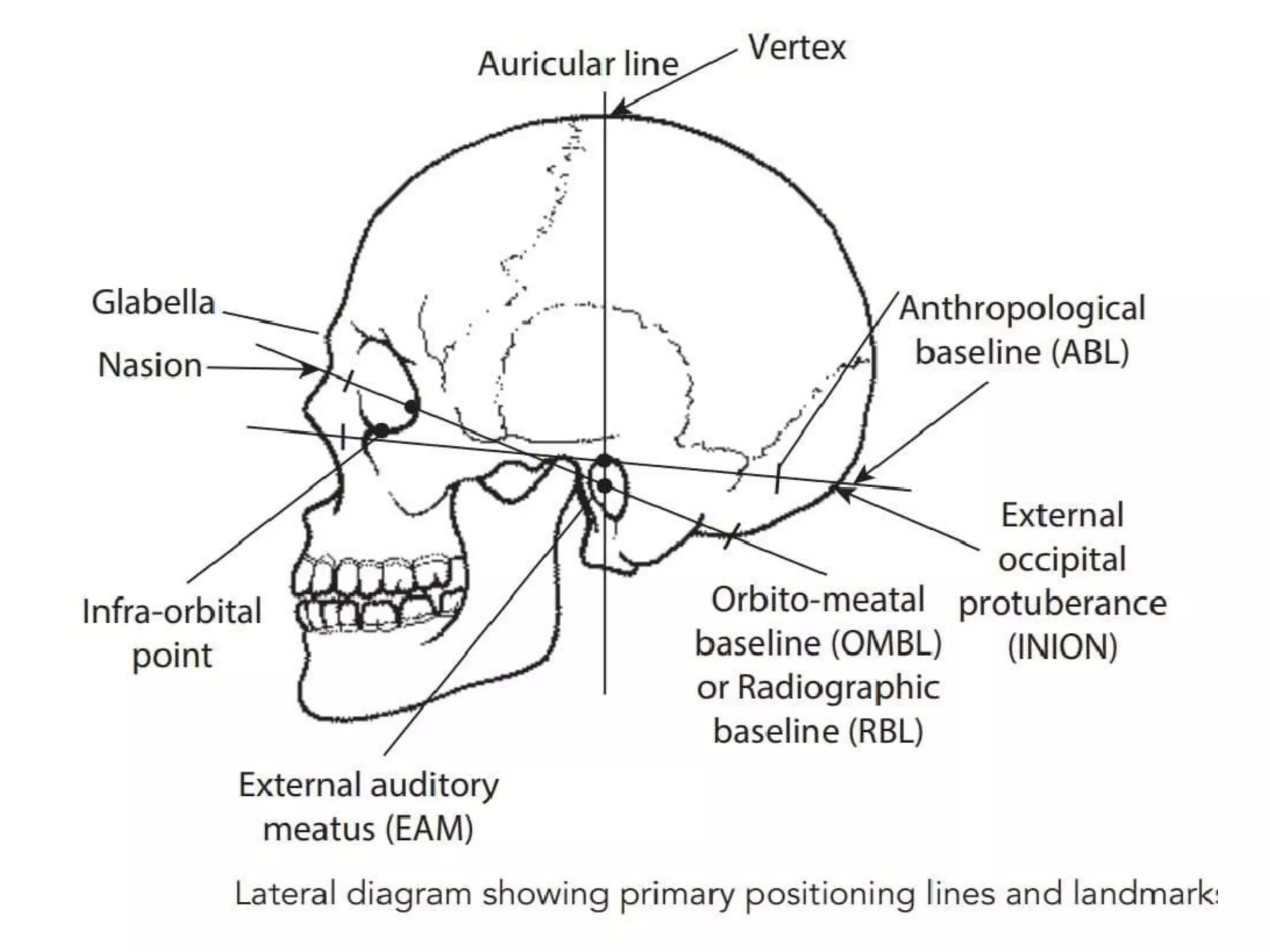
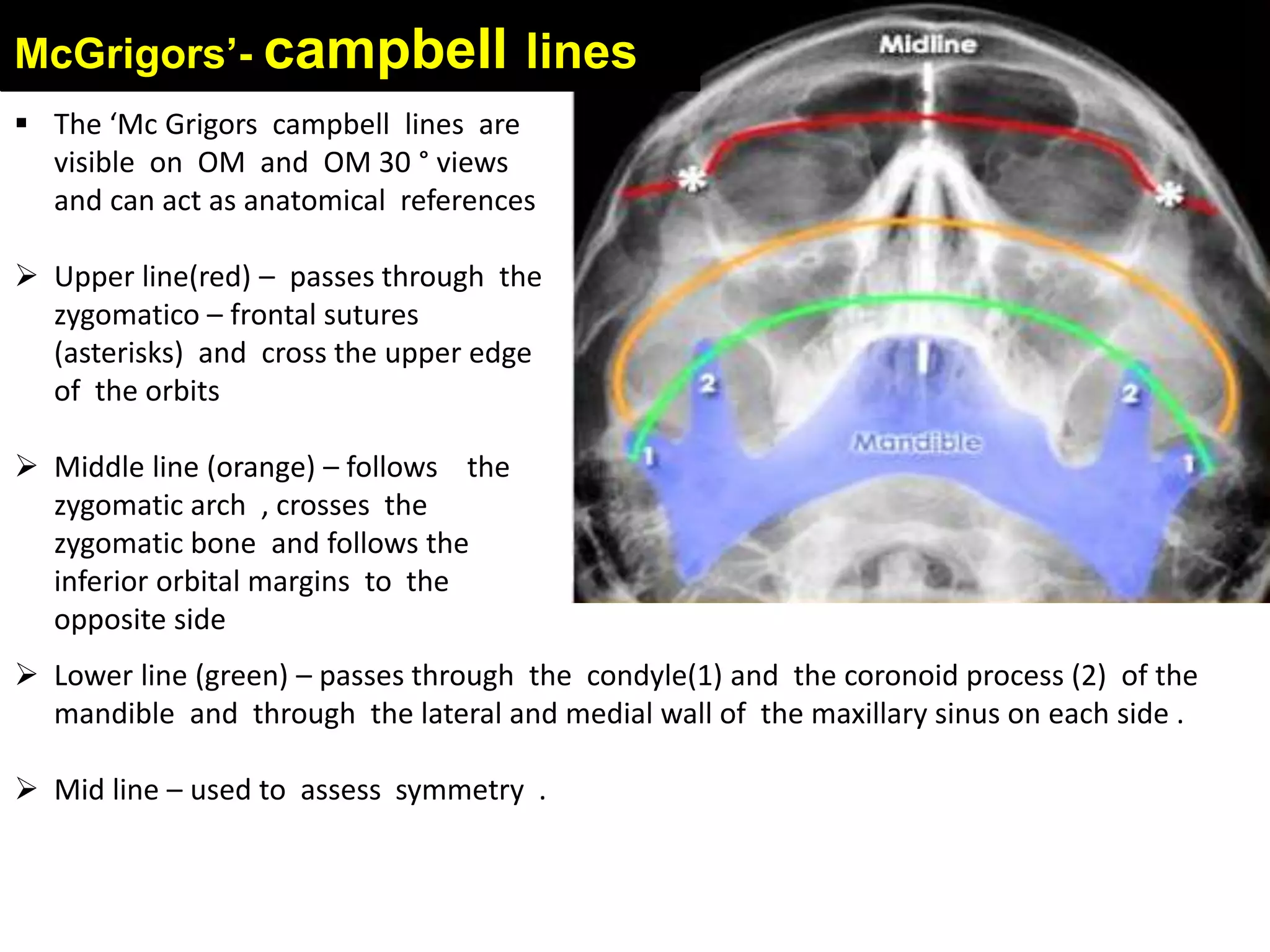
2) Important anatomical landmarks and lines are highlighted to guide fracture identification, including the McGrigor-Campbell lines.
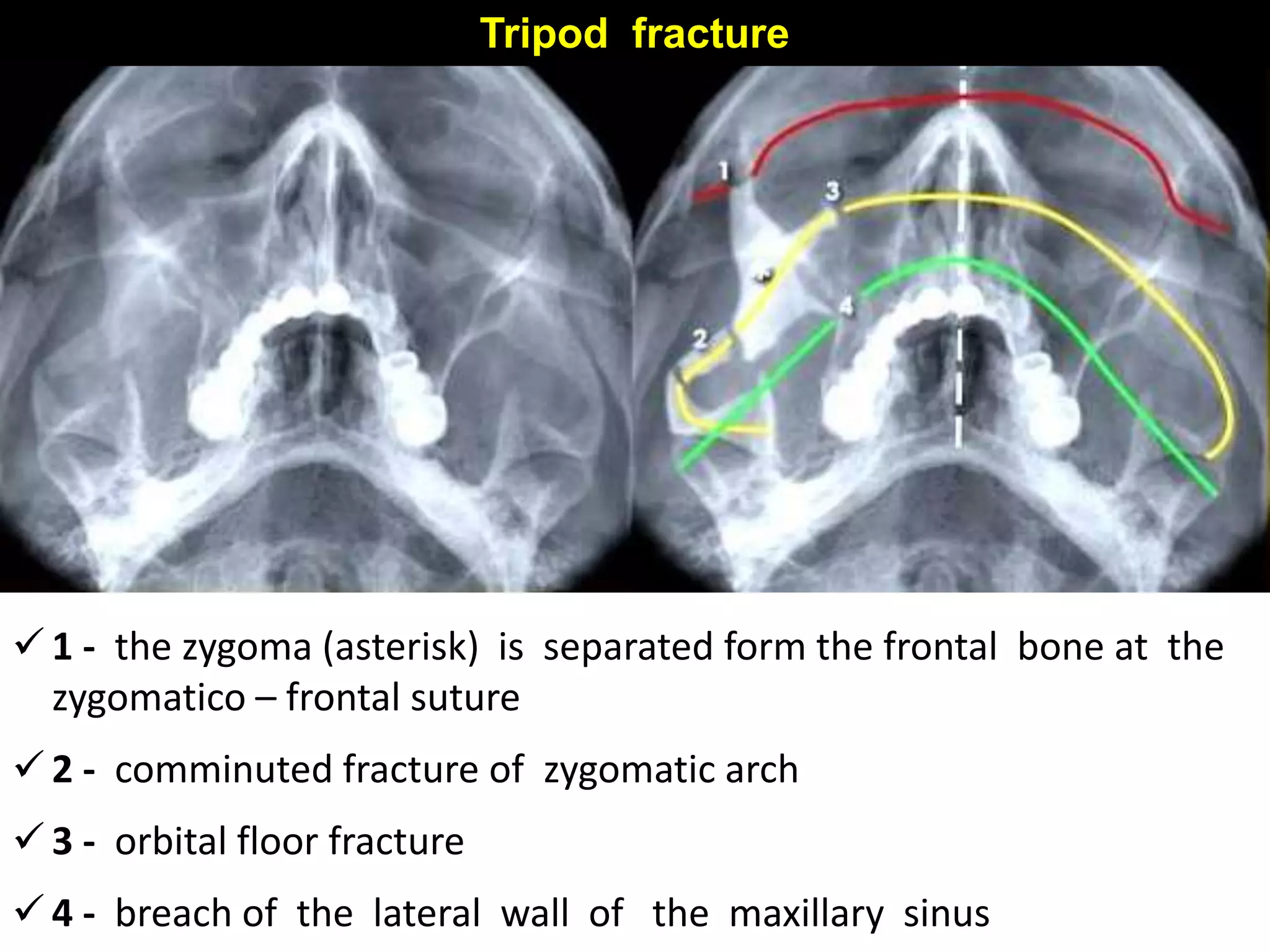
3) Common facial fracture patterns such as isolated zygomatic arch fractures, "tripod" fractures, and orbital "blowout" fractures are demonstrated along with their radiographic signs. The summary also emphasizes looking for multiple fractures in cases of mandible fractures.
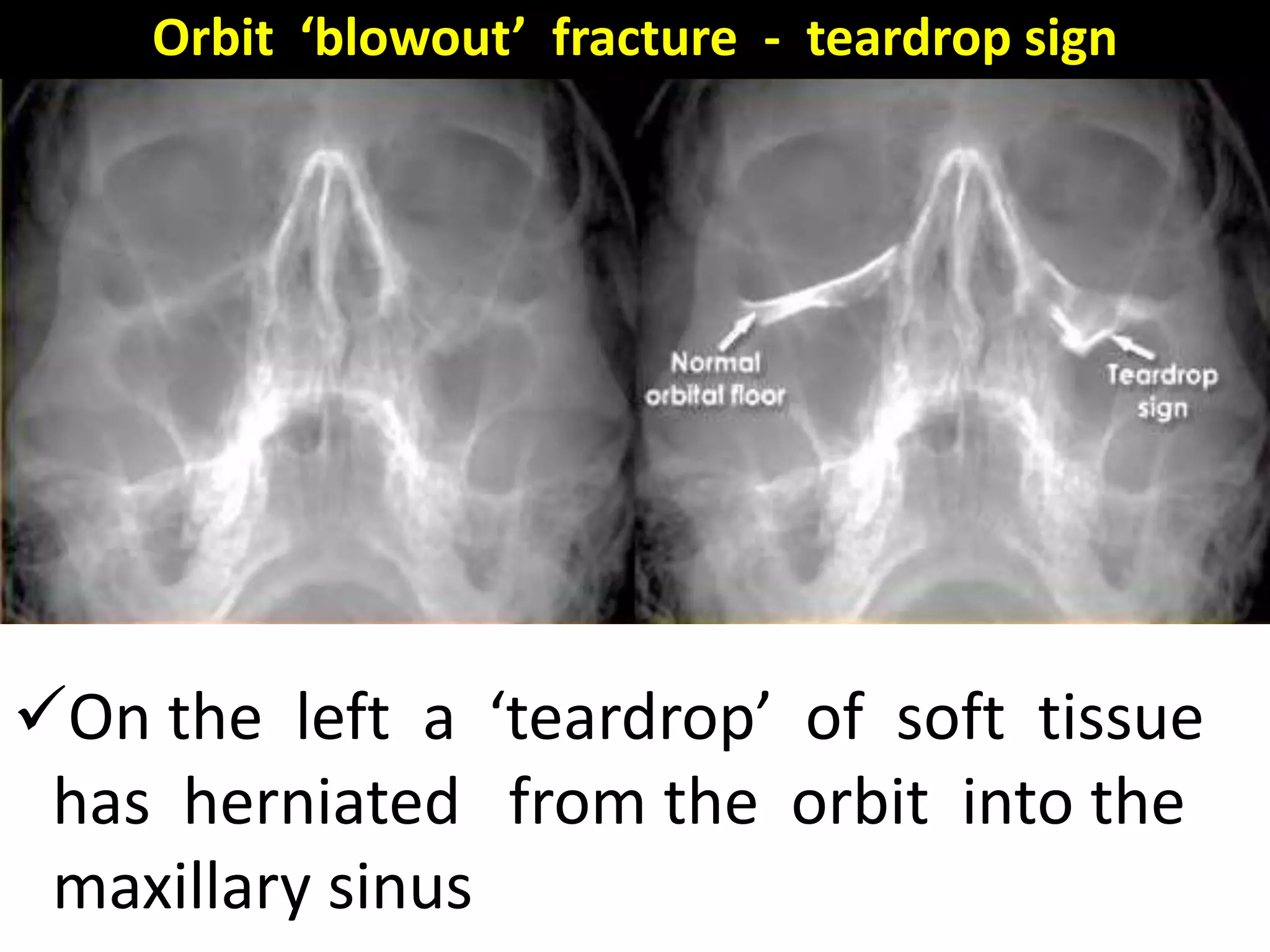
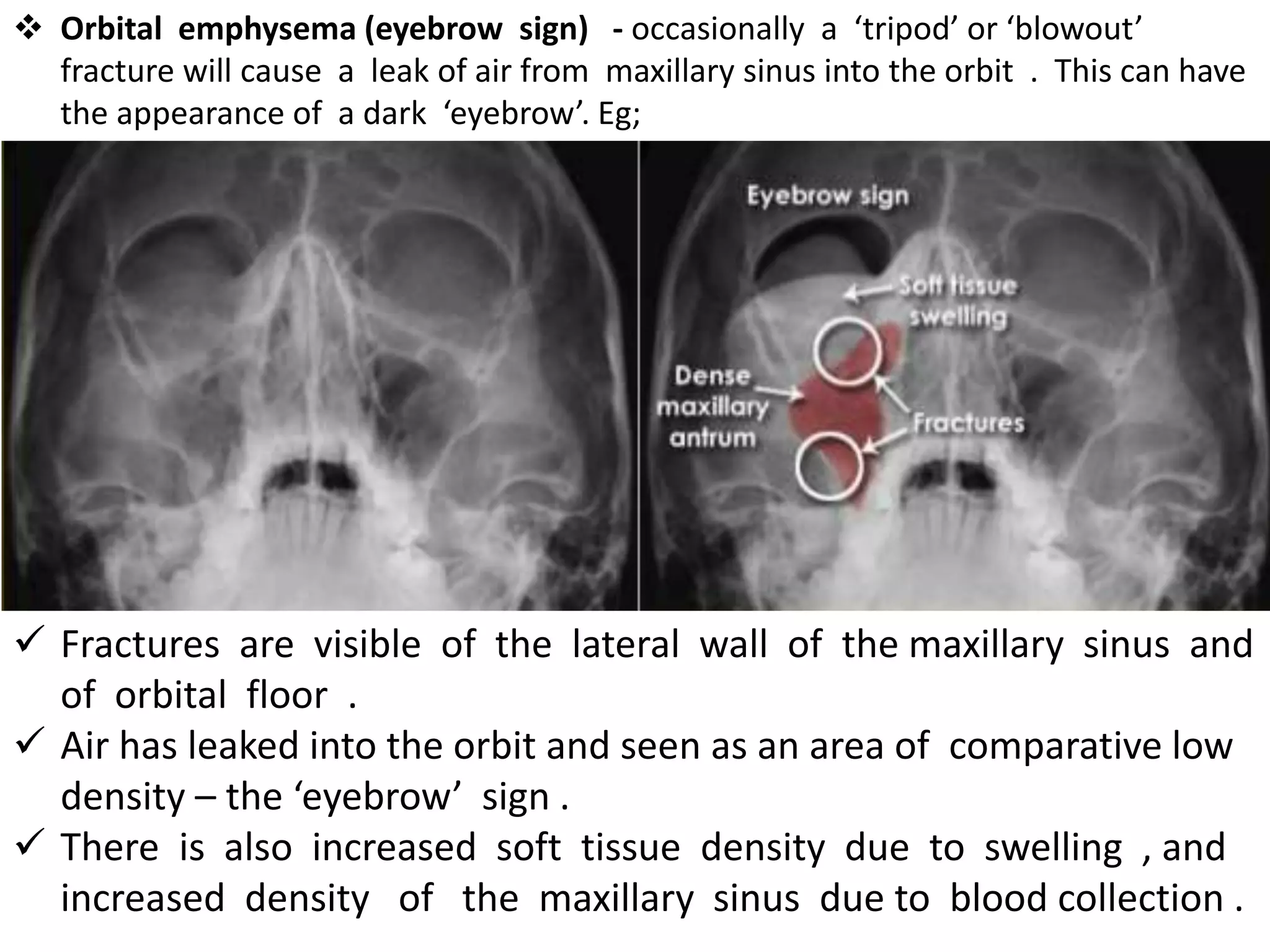
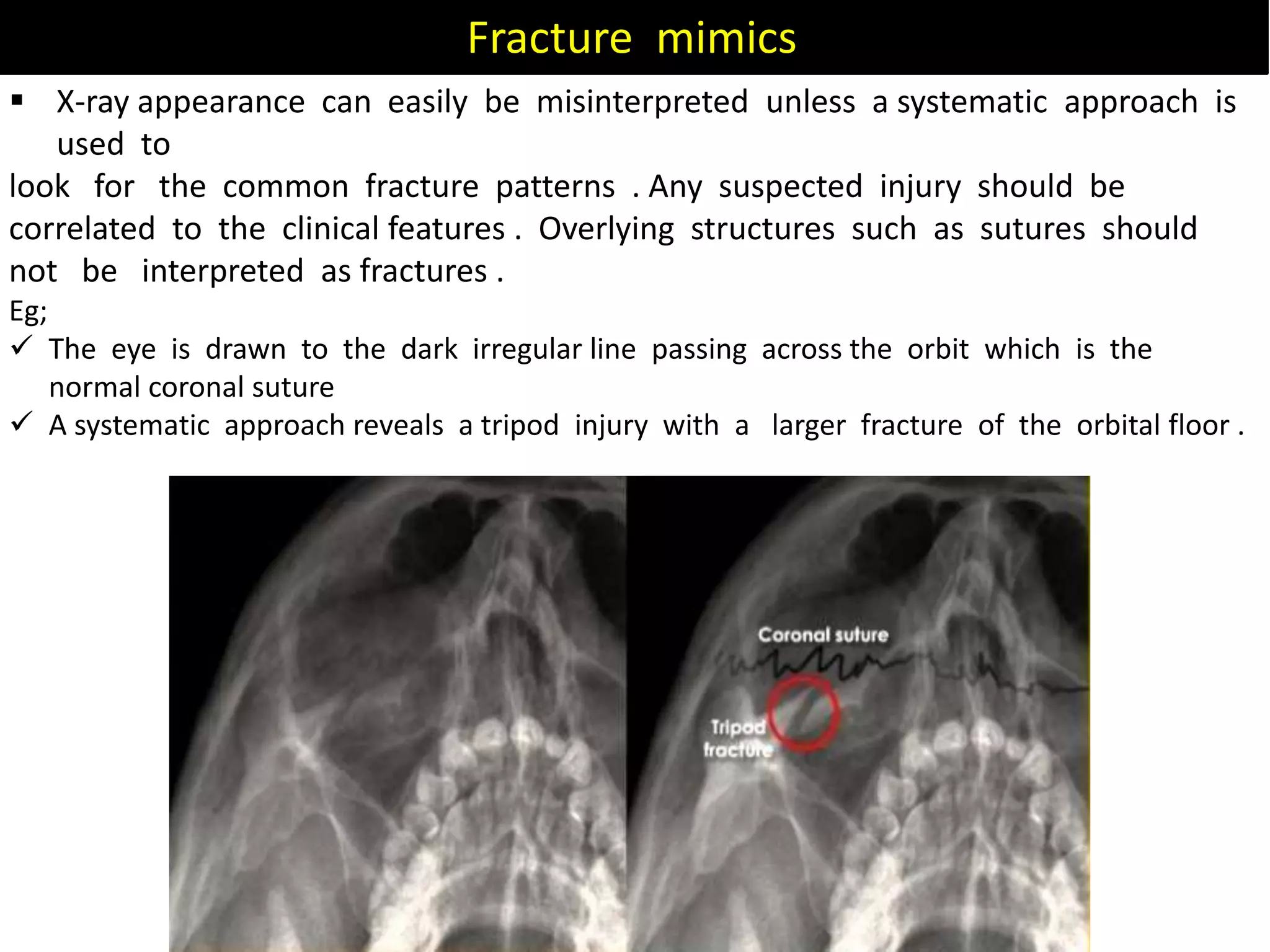
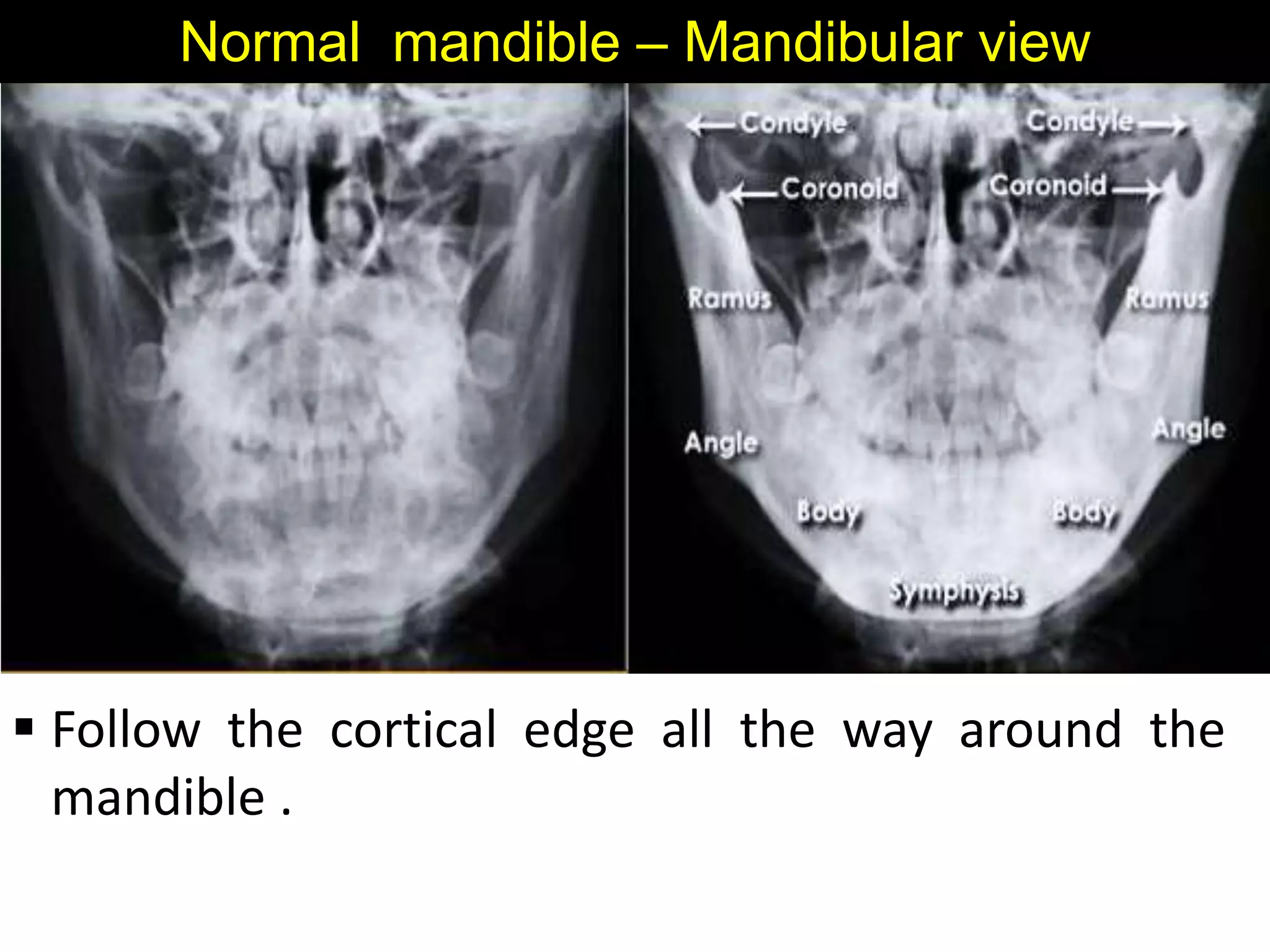
![Palatine bone
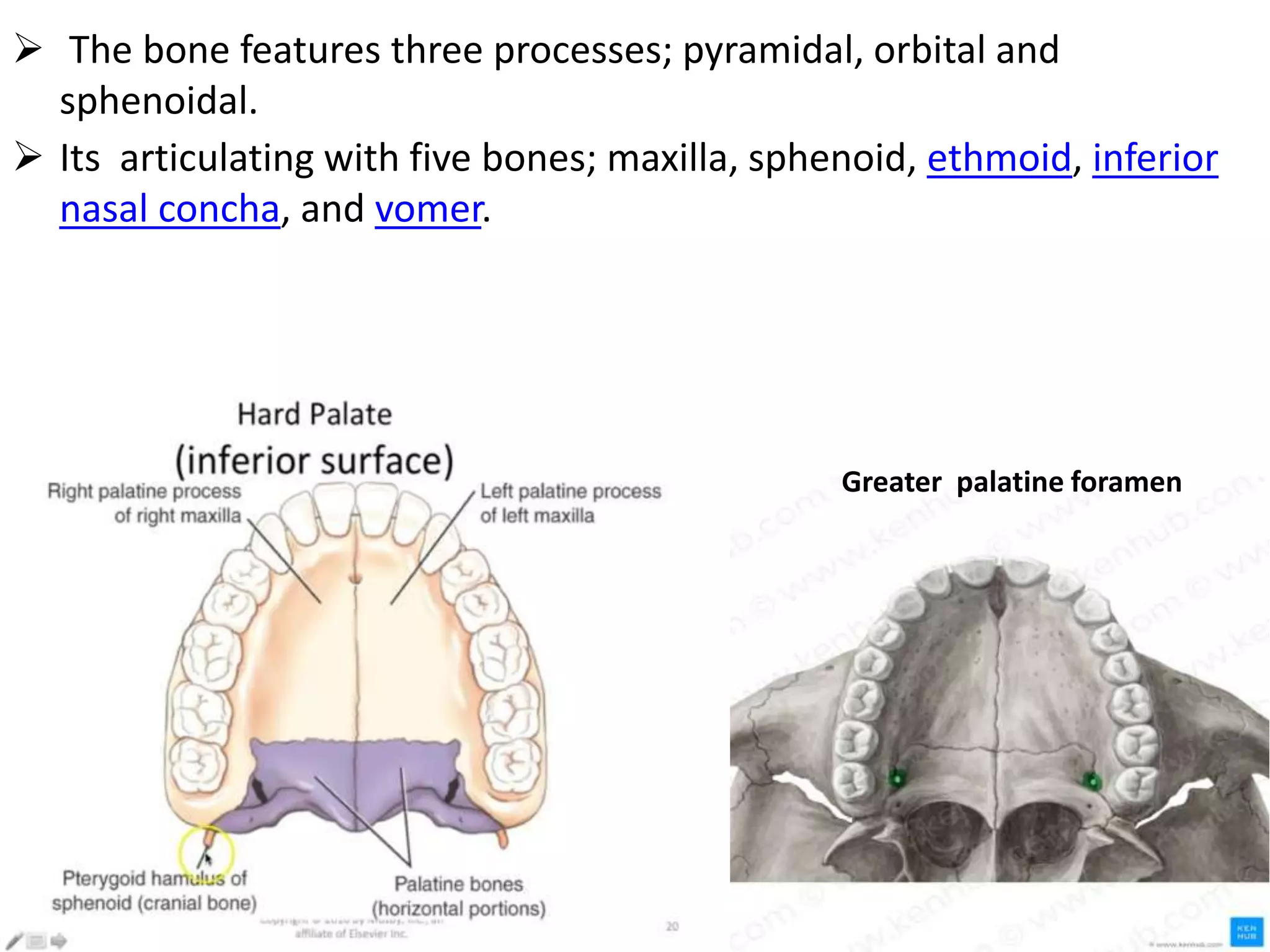
Two L – shaped bone composed of vertical and horizontal plates
Horizontal plates articulate with maxillae to complete the
posterior fourth of bony palate (roof of mouth)
vertical portion extend upward between maxilla and the pterygoid
process of the sphenoid in posterior nasal cavity
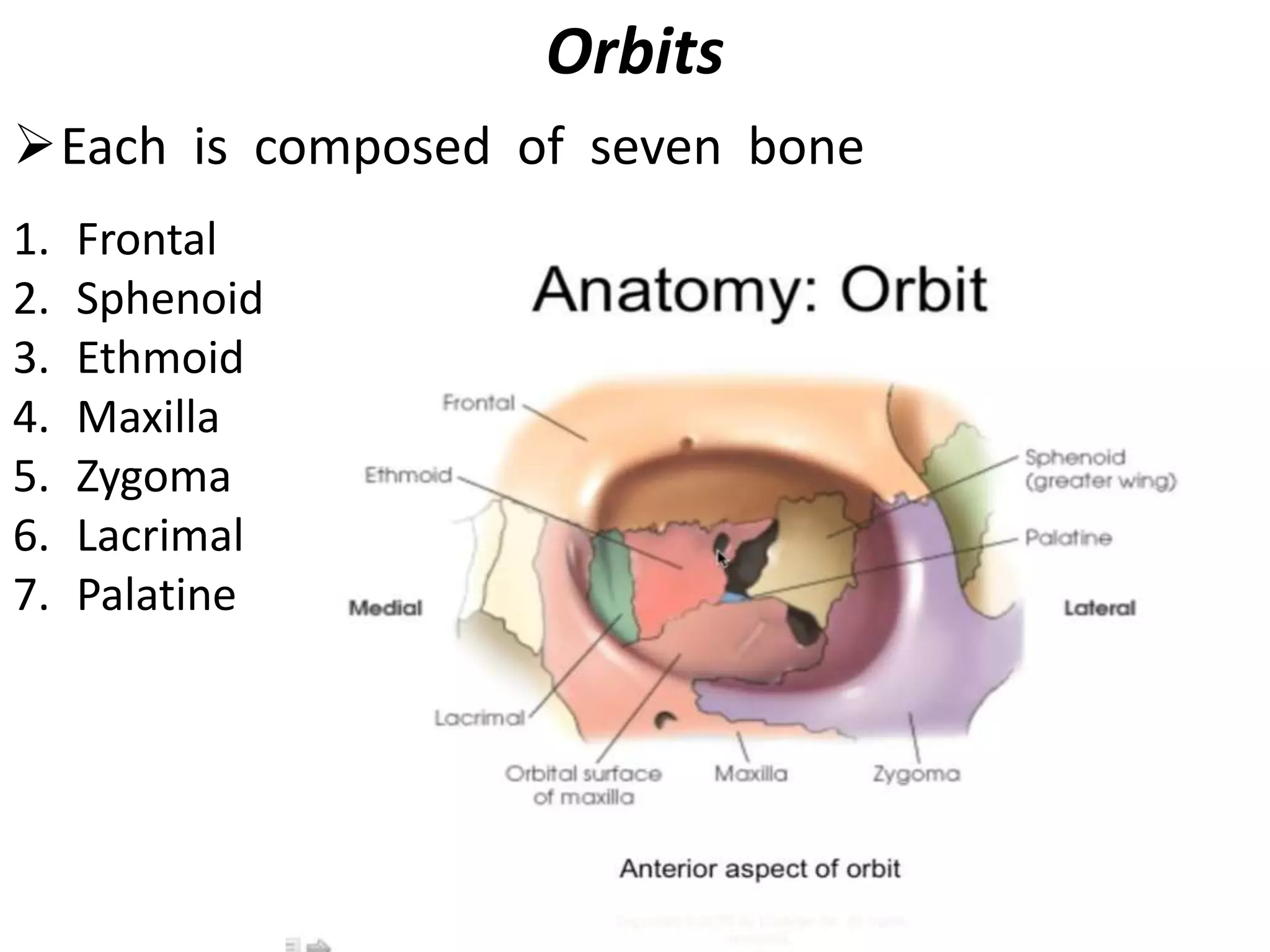
Palatine bone contributes to the walls of three cavities:-
1] The floor and lateral wall of the nasal cavity;
2] The roof of the mouth,
3] The floor of the orbit.](https://image.slidesharecdn.com/anatomyandimageinterpretationoffacialbone-210409020406/75/Anatomy-and-image-interpretation-of-facial-bone-14-2048.jpg)














































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










