
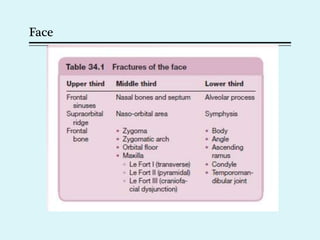


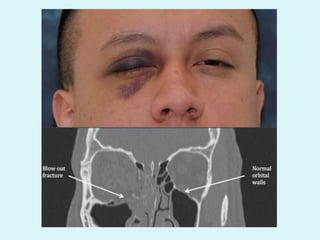
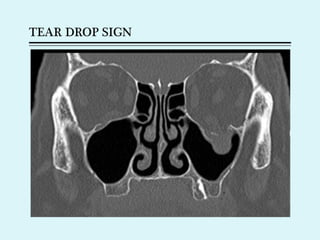
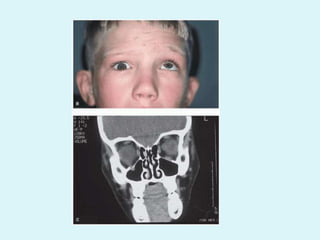
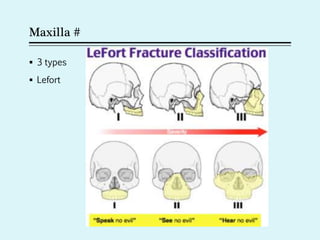
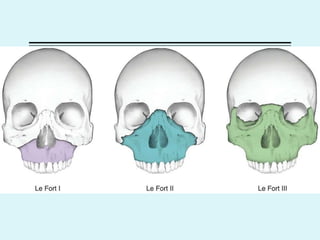
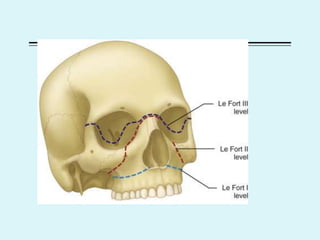
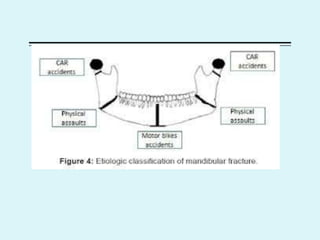
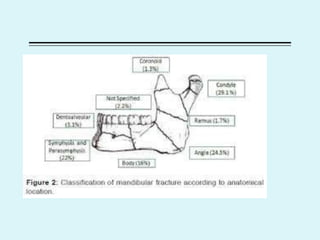



This document discusses trauma to the face, including causes such as automobile accidents and sports injuries. It describes the management of soft tissue injuries, bone fractures, and other conditions affecting the upper, middle, and lower thirds of the face. Specific fractures discussed include the nasal bone, orbital floor, zygoma, maxilla, and mandible. Diagnosis involves physical examination, x-rays, and CT scans. Treatment depends on the location and severity of the injury, and may involve closed or open reduction of fractures as well as fixation with wiring or plates.























































































