Downloaded 20 times
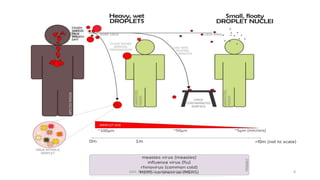
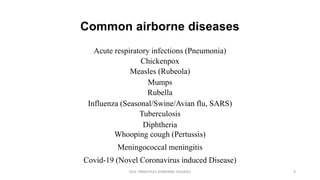


This document discusses airborne diseases, defined as illnesses caused by pathogens suspended in the air that can be transmitted through respiratory droplets or aerosols. It outlines the transmission methods, common airborne diseases, their clinical features, diagnosis, treatment, and prevention strategies, emphasizing the impact of environmental and social factors on infection rates. Additionally, it highlights regulations and health programs aimed at controlling and preventing airborne diseases.



































































