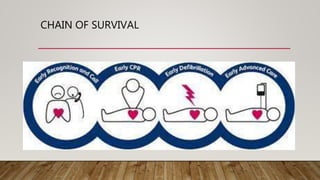
The document outlines the principles and protocols of Advanced Cardiac Life Support (ACLS) and Basic Life Support (BLS), emphasizing the importance of timely intervention and appropriate assessment during cardiac emergencies. It covers the chain of survival, methods of defibrillation, the anatomy of the heart, and medications used during ACLS procedures. Key techniques and guidelines for effective CPR and defibrillation are also detailed, alongside potential risks and best practices for various patient scenarios.