Downloaded 74 times
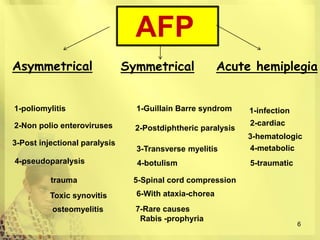
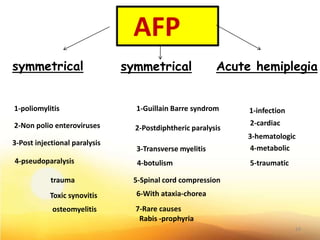

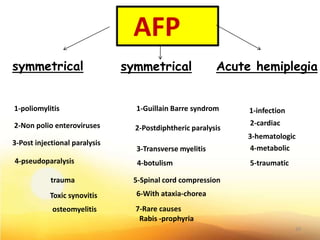
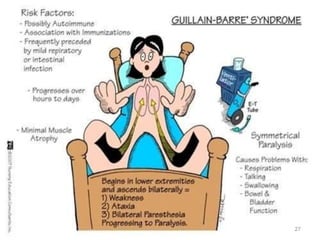

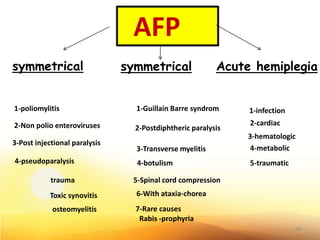
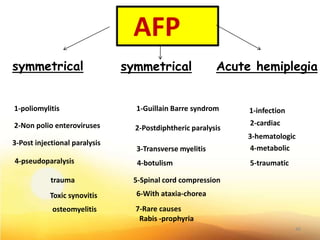


1. Acute flaccid paralysis (AFP) can present asymmetrically or symmetrically. Asymmetrical AFP may be caused by poliomyelitis or non-polio enteroviruses, while symmetrical AFP may be Guillain-Barré syndrome or transverse myelitis. 2. Important considerations in the evaluation of a child with AFP include differentiating acute infections from post-injection paralysis, obtaining a thorough history of recent vaccinations or infections, and ruling out treatable causes with imaging or lumbar puncture when indicated. 3. Proper management depends on the stage of illness, with the acute stage prioritizing isolation and prevention of paralysis progression, the restoration stage involving physi























































































