Download as PDF, PPTX
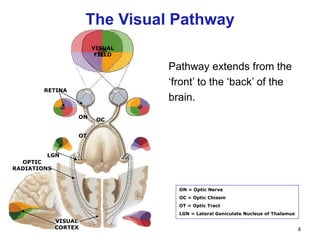
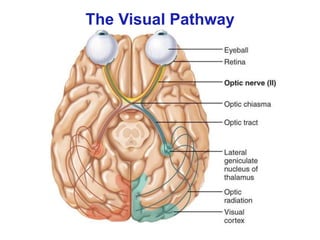

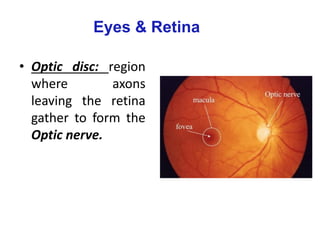
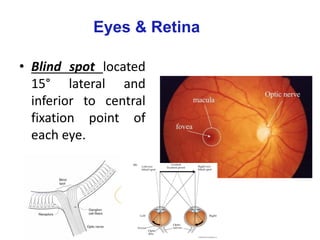
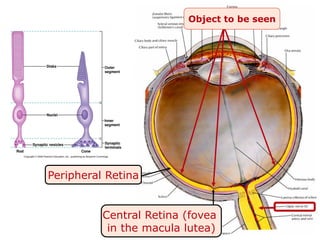
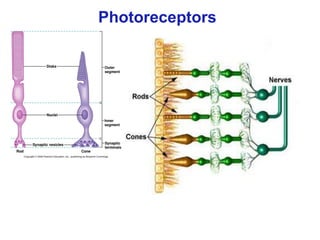
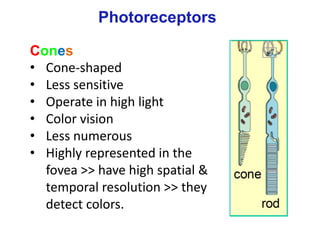
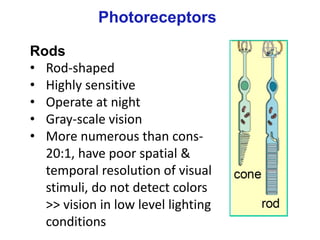
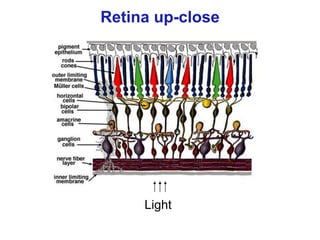
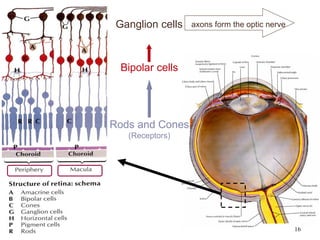
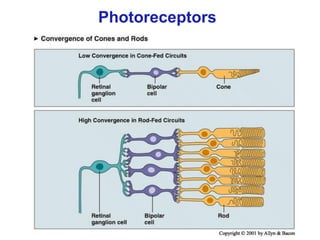
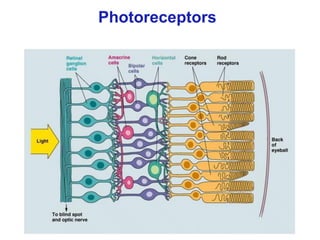
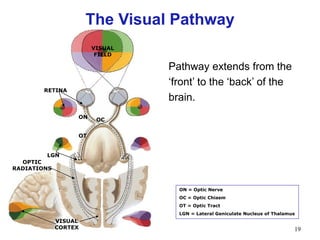
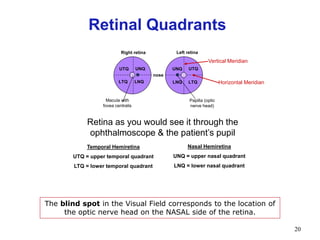
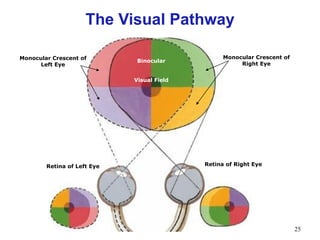
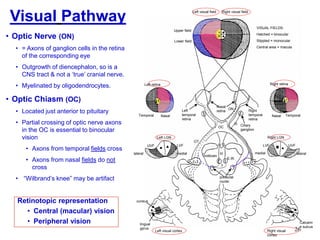
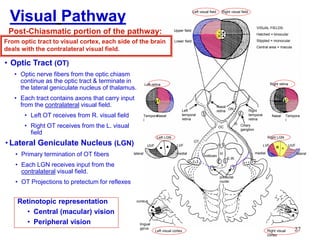
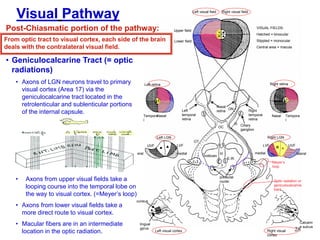
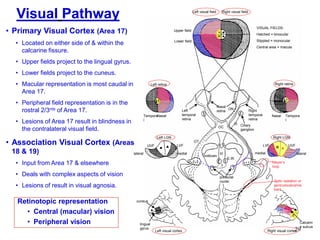
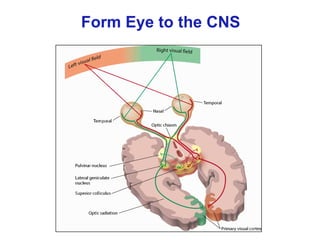
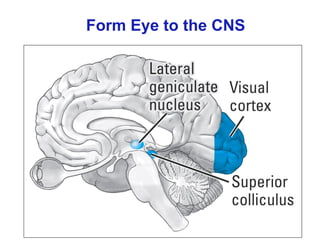
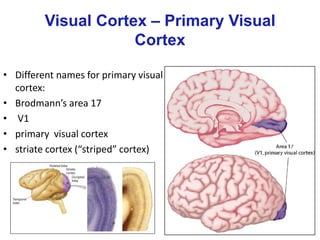
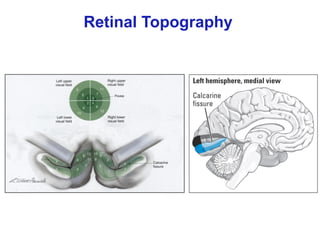
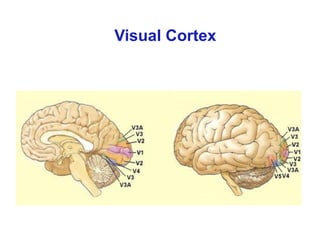
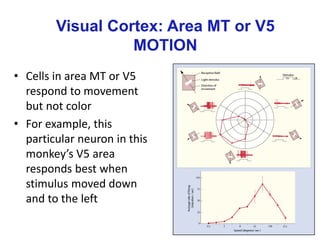
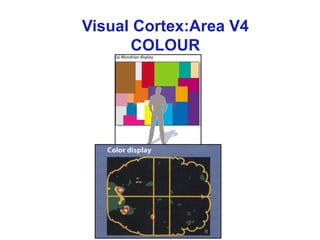
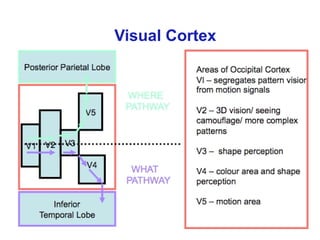
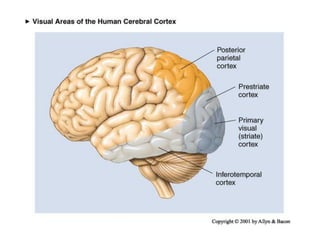
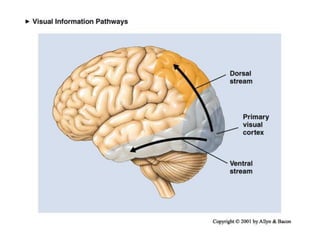
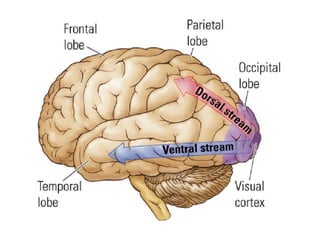
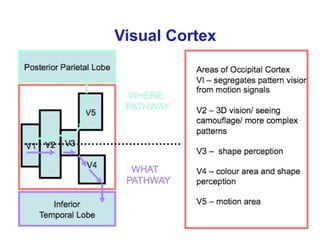
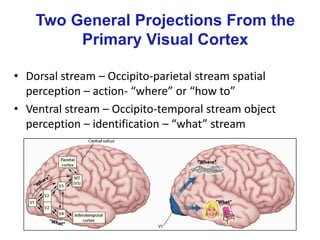
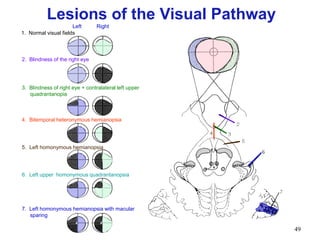
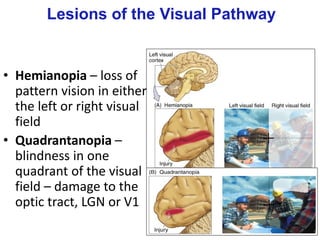


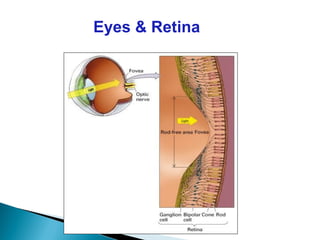
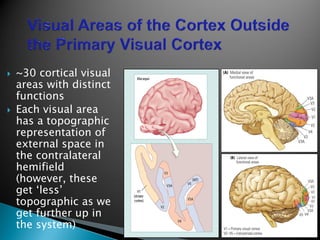
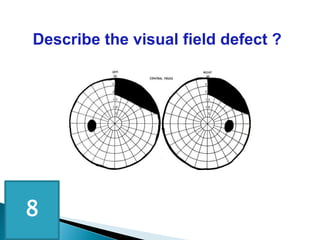
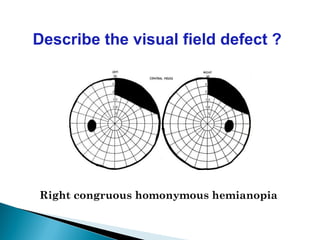

The document outlines the anatomy and functionality of the afferent visual pathway, detailing the structures involved from the retina to the visual cortex, including the optic nerve, optic chiasm, and lateral geniculate nucleus. It also discusses the types of visual field defects related to lesions in the visual pathway and introduces concepts like monocular and binocular vision, different types of photoreceptors, and visual processing streams. Lastly, it highlights various disorders connected to the visual pathway, including visual agnosia and color perception deficits.










































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
