ATOMIC ENERGY REGULATORYBOARD(AERB)
• It was constituted on November 15, 1983 under the Atomic Energy Act 1962 and environmental
(protection) act 1986
• It is an apex body that regulates the use of ionizing radiation in the country.
• The mission of AERB is to ensure that the use of ionizing radiation and nuclear energy does not cause
undue risk to health and environment
3.
Roles and Responsibilities
•Licensee(usually the Head of the department)
• Ensures AERB license, equipment approval and compliance
• Radiation Safety Officer (RSO)
• Monitor exposure, train staff and to manage incident reports
• Radiation workers
• Should wear radiation protective equipment with dosimeters, and follow
safety protocols
4.
Responsibility of Licensee
1.Regulatory Compliance: Follow all AERB rules, license conditions, and notify AERB of any changes.
2. Radiation Protection: Implement a radiation safety program; appoint an AERB-approved Radiation
Safety Officer (RSO).
3. Training: Ensure all radiation workers are trained and competent.
4. Monitoring: Monitor radiation exposure of workers (e.g., TLD badges) and workplace areas;
maintain dose records.
5. Record Keeping: Keep detailed records of sources, personnel, training, incidents, and safety
checks.
5.
• 6. EmergencyPreparedness: Have a response plan; conduct drills; report incidents
promptly to AERB.
• 7. Safe Handling & Disposal: Store, handle, transport, and dispose of sources safely
and as per AERB norms.
• 8. Quality Assurance: Maintain equipment calibration and performance through
regular QA checks.
• 9. Security: Ensure physical security of radioactive materials to prevent theft or misuse.
• 10. Communication: Report any abnormal events and stay in regular contact with AERB
for renewals, changes, or decommissioning.
6.
• It isthe responsibility of the owner (employer) of the facility for
providing personnel monitoring devices (TLD badges) to radiation
workers such as X-ray Technologists and medical practitioner(s)
and
• to ensure that dose received by radiation worker(s) are as low as
reasonable achievable (ALARA).
7.
Radiation Safety Officer(RSO)
• Ensure compliance with AERB safety norms.
• Monitor staff radiation exposure (TLDs).
• Conduct safety training and awareness.
• Oversee equipment safety and QA checks.
• Perform area radiation surveys.
• Maintain safety records and documentation.
• Report incidents to AERB.
• Advise the licensee on radiation safety.
8.
Radiation workers
• FollowSafety Procedures: Adhere to all radiation safety protocols.
• Wear TLD Badge: Use personal dosimeter correctly and consistently.
• Use Protective Gear: Wear lead aprons, thyroid shields, etc., as required.
• Limit Exposure: Minimize time near X-ray source and maximize distance.
• Report Issues: Notify RSO of any unsafe conditions or incidents.
• Attend Training: Participate in radiation safety training sessions.
• No Unauthorized Use: Operate equipment only if trained and authorized.
• Follow Instructions: Comply with RSO and licensee’s safety directions.
9.
RADIATION SAFETY PROGRAMME
•The main goals of this programme are
• Prevent detrimental tissue reactions (deterministic effects)
• Limit or minimize the probabilistic effects to acceptable levels
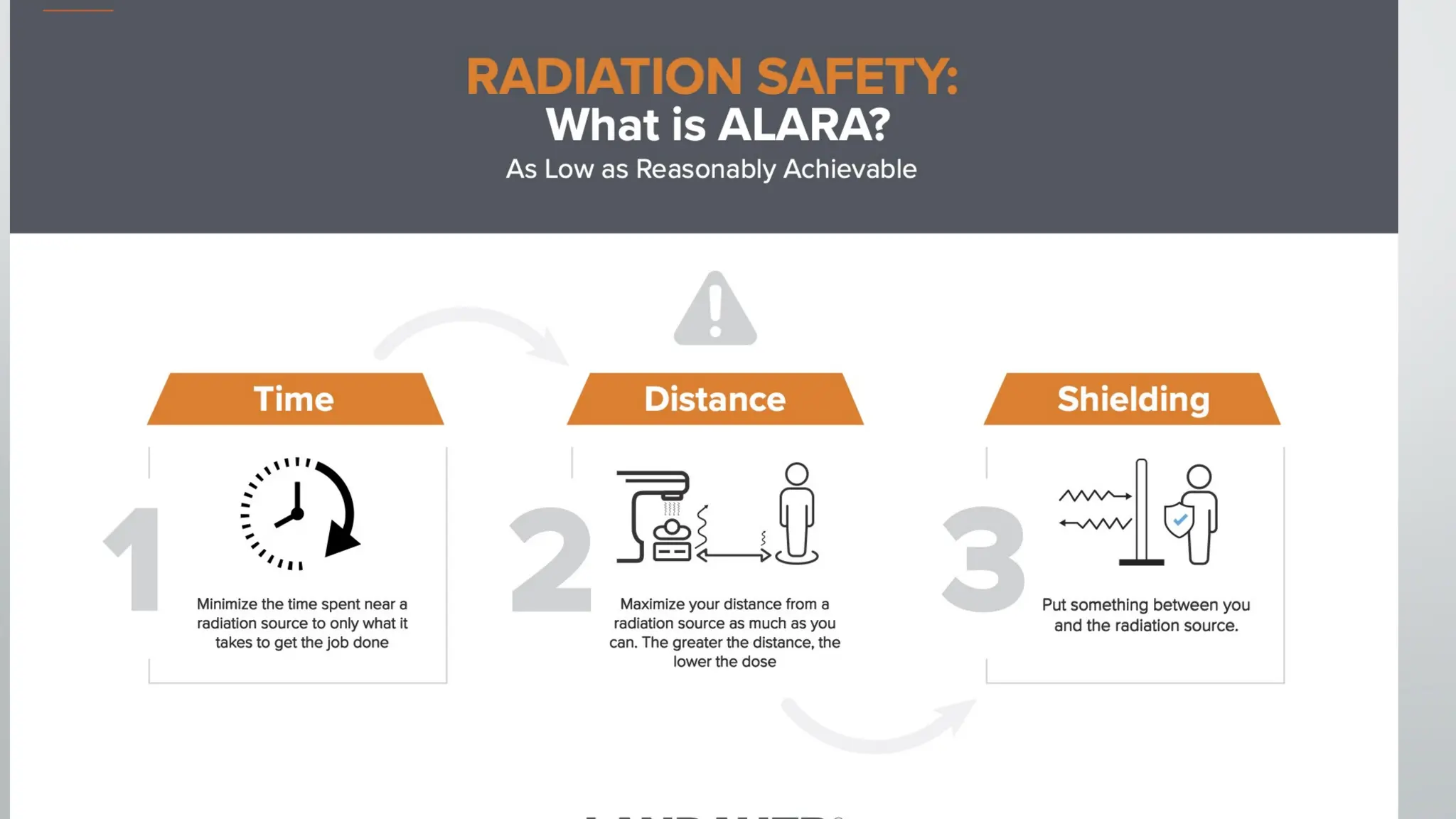
ALARA PRINCIPLES FORRADIATION SAFETY
•Time
• Directly proportional to exposure rate
•Distance
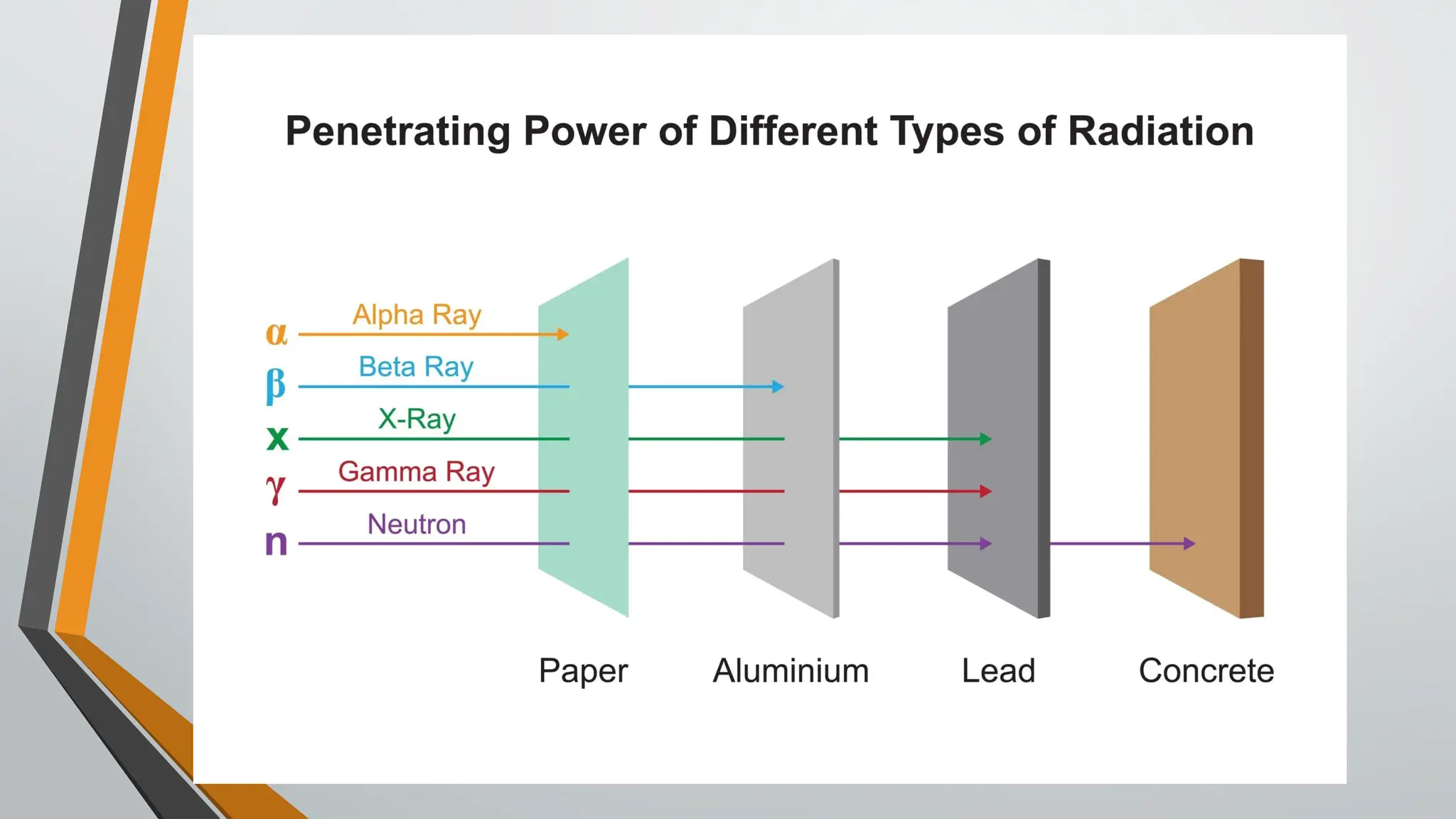
•Shielding
• Usage of shielding materials like lead, concrete
14.
Core principles forradiological protection
• JUSTIFICATION for radiation usage
• OPTIMISATION ( on the principle of ALARA )
• DOSE LIMITATIONS and dosages from different modalities
15.
JUSTIFICATION
• The mostcommon type of ionizing radiation used in diagnostical
imaging all over the world are X-rays since its discovery.
• While there are obvious benefits from medical uses of X-rays , however
there are well established health risks from radiation if improperly
applied. Hence every medical procedure involving radiation needs to be
justified.
• Diagnostic x-ray examinations contribute the largest fraction to
population dose from man made radiation sources.
16.
OPTIMIZATION
• Ionizing radiationcauses biological changes in the exposed person at
the cellular level.
• Hence the doses to the occupational workers shall be kept as low as
reasonably achievable(ALARA)
• Doses to patients shall be optimized to minimize radiation exposure so
that proper imaging can be obtained with minimal radiological risk.
17.
DOSE LIMITS
PART OFTHE BODY OCCUPATIONAL EXPOSURE PUBLIC EXPOSURE
Whole body (Effective dose) 20 mSv/year averaged over 5
consecutive years
30 mSv in any single year
1 mSv/y
Lens of eyes
(Equivalent dose)
150 mSv in a year 15 mSv/y
Skin
(Equivalent dose)
500 mSv in a year 50 mSv/y
Extremities - (Hands and Feet)
(Equivalent dose)
500 mSv in a year -
For pregnant radiation workers, after declaration of pregnancy
1 mSv on the embryo/fetus should not exceed
18.
Types of RadiationGenerating
Equipment: (RGE)
• Computed Tomography
• Interventional Radiology
• Radiography (Fixed/Mobile)
• C-Arm/ O-Arm
• Mammography
• Bone Mineral Density tests
• Dental (Intraoral/OPG/CBCT)
Note: MRI and Sonography (Ultrasound) or non-ionizing RGE do not come under
purview of AERB regulations
20.
Factors in dosereduction
• Following operational safety
• Reduce the time spent near the X-ray source (eg. reduce
fluoroscopy procedure time)
• Increase the distance from the X-ray source
• Interpose a shielding material between X-ray source and
Operator- by the use of radiation protection accessories
21.
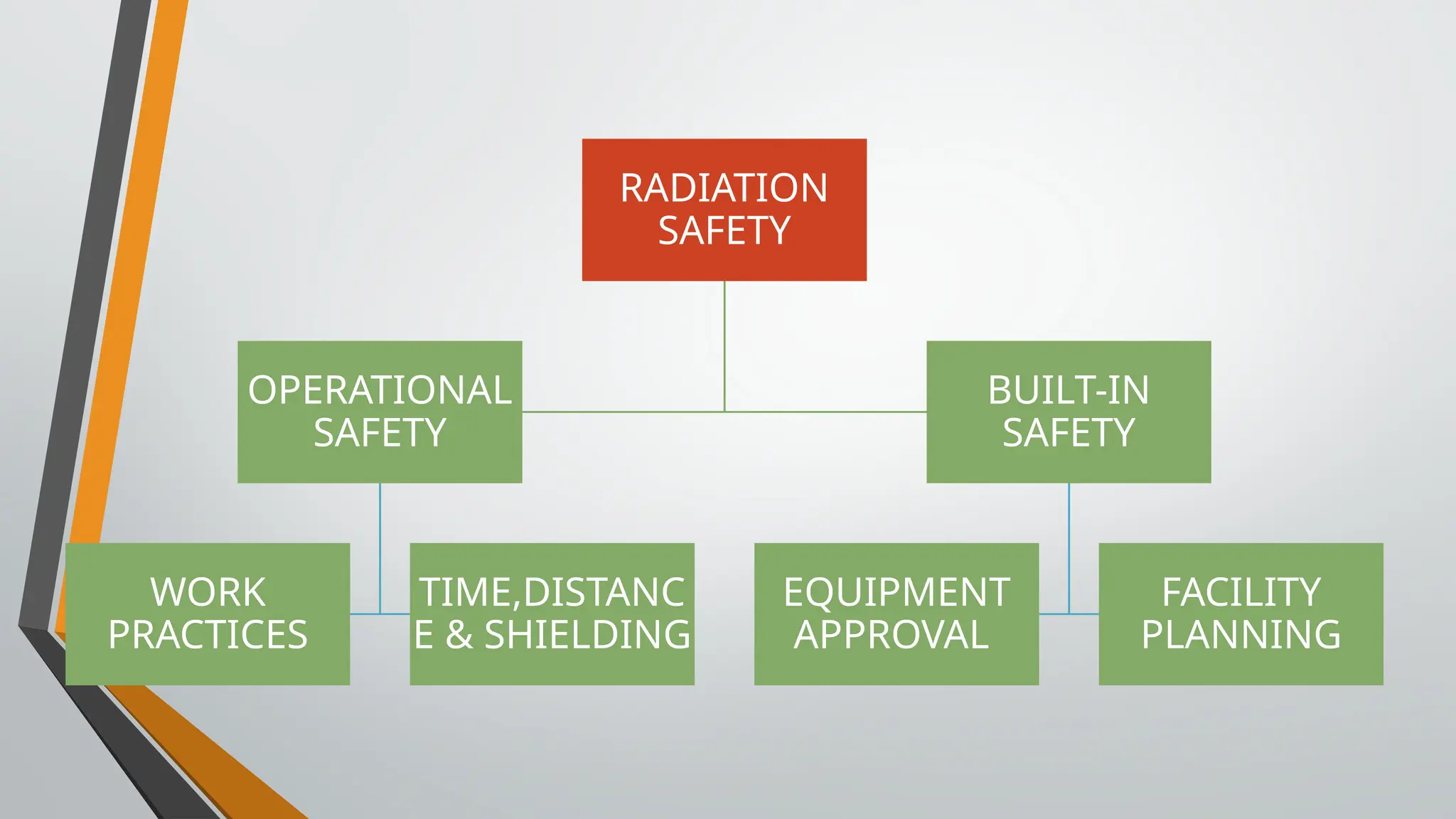
Operational Safety
• Componentsof operational safety
• Handling of equipment by certified personnel
• Use of protective accessories like Mobile Protective Barrier, Lead Apron,
Organ shield etc.
• Usage of Personnel monitoring devices (TLD)
• Preventive maintenance and periodic Quality Assessment(QA) of equipment
• Updating with the current regulatory requirements
22.
Protection of Staff/Operator
•By the usage of lead apron (0.25 mm lead
equivalent), radiation dose would be reduced by
more than 90 %
• Use ceiling suspended screens, lateral shields and
table curtains- must for interventional radiology
procedures.
• 0.25 mm Lead equivalent glass eyewear with side
protection
23.
Minimizing radiation exposure
•Always collimate to the area of interest, the amount of tissue the beam
is allowed to irradiate is directly proportional to the scatter radiation is
produced.
• Avoid holding of infirm patient by staff, provide protective apron to the
attendants while holding such patients.
• During use of mobile x-ray equipment ,stand at least 6 feet away
from the patient and wear lead apron.
24.
Shielding with C-ARM& Fluoroscopy
• C-Arm positioning greatly influences the amount of scattered
radiation
• ideally, C-Arm should be positioned with the image intensifier
above the patient and the x-ray tube below,
• This directs scatter toward the operator’s feet instead of the
head, since the highest scatter component is the scatter reflected
from the primary beam initial impact on the patient.
• When using fluoroscopy across the patient, the operator should
be positioned on the same side of the patient as the image
intensifier, not the x-ray tube side.
26.
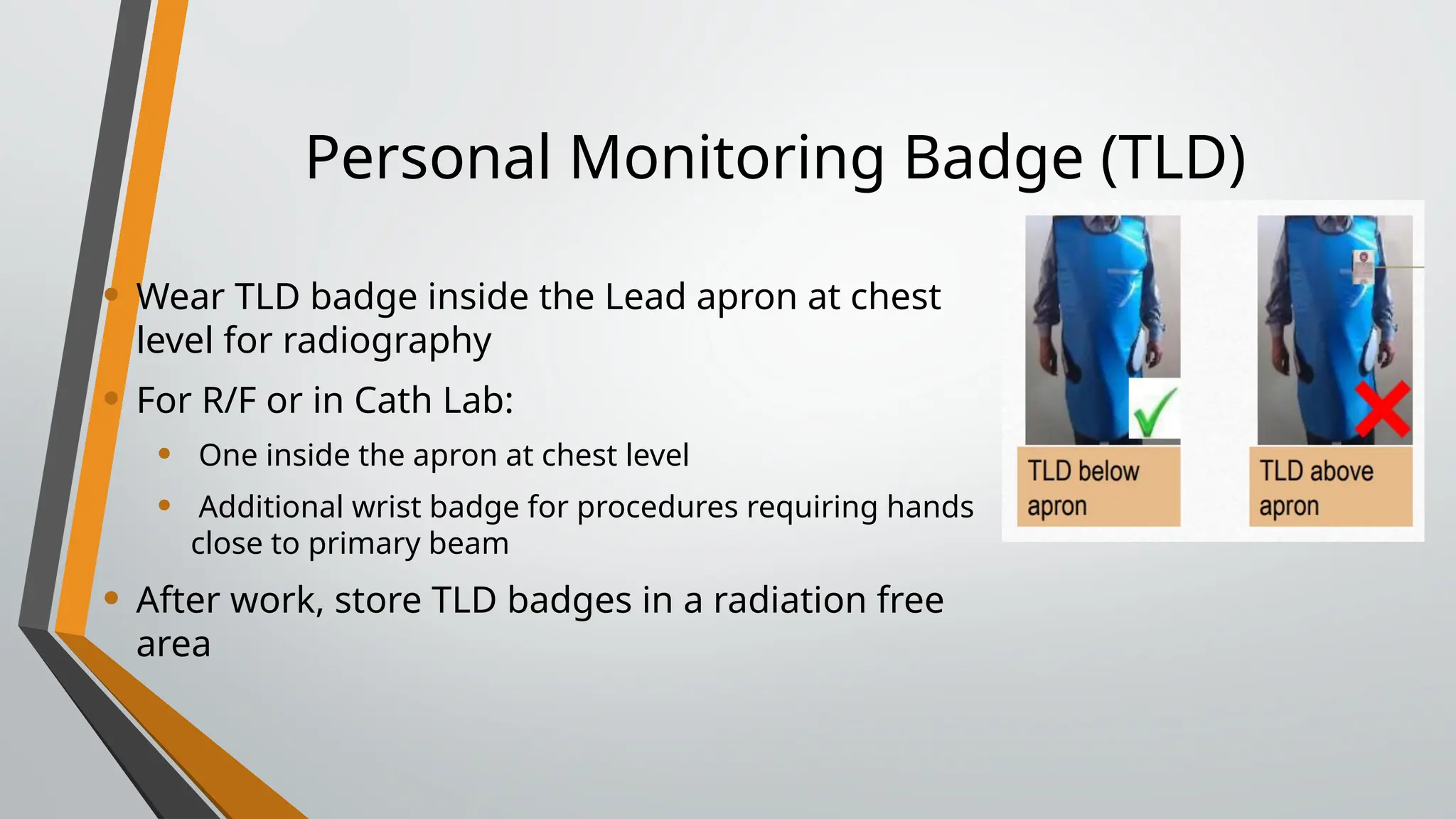
Personal Monitoring Badge(TLD)
• Wear TLD badge inside the Lead apron at chest
level for radiography
• For R/F or in Cath Lab:
• One inside the apron at chest level
• Additional wrist badge for procedures requiring hands
close to primary beam
• After work, store TLD badges in a radiation free
area
28.
Patient dose management
•Justify the procedure
• Ask for records of previous diagnostic procedures
• Plan the procedure (right patient, right contrast, purpose of
scan/investigation)
• Inform patient about his/her procedure
• Know well about your equipment settings
• Ensure only qualified and trained operator should operate the
equipment
29.
Patient Protection duringprocedure
Radiation safety during x-ray examination of patient is ensured by
• Limiting the total “beam–on” time & avoiding oblique lateral projections
• Prior to exposure, collimate the x-ray beam to the area of interest to
avoid post-exposure cropping of the image
• Use of correct exposure protocols for patient examinations including
paediatric protocols and selecting low dose rate protocol
• Monitoring of DLP in CT and DAP values for IR procedures and record-
keeping of patient’s doses for CT and IR procedures.
30.
Radiation protection ofpaediatric patients
• Keep in mind for paediatric examinations
• Grid should not normally be used
• Use equipment with high power i.e. higher mA and shortest
time
• Use thyroid, gonad shields & immobilization devices
• Scan only the indicated region ; multiphase scanning is usually not necessary
for children unless specifically indicated
ONLY EXPOSE THE AREA OF
INTEREST
31.
Protective Devices –Quality Control
• All lead equivalent vinyl material (aprons, gloves) should comply with
relevant international standards. They should be tested at purchase
and regularly thereafter, at least every 2 years.
• Incorrect storage may lead to cracks in the shielding but this may not
be detectable by visual inspection alone
• A simple test is to examine the devices using fluoroscopy (at about 60
kVp). The use of automatic dose rate or automatic brightness controls
should be avoided.
32.
Quality Assurance testing
•Carrying out Quality Assurance testing of each & every X-ray
equipment once in two years is highly recommended as
• Improves imaging standard
• Increase the Life of the X-ray tube/ equipment by avoiding retakes
• Useful in reduction of unnecessary dose to patient and staff
#2 The major objectives are to develop and publicize specific codes and guides, which will deal with the radiation safety aspects of various applications of radiations. It will also issue authorization related to site, design, manufacture, construction, commissioning, operation, maintenance, and decommissioning and disposal of radioactive sources
#7 Regulatory Compliance
Ensure radiology practices follow AERB safety codes and license conditions.
Radiation Protection
Implement and supervise radiation safety measures for staff, patients, and the public.
Personnel Monitoring
Ensure proper use of TLD badges and maintain dose records.
Training & Awareness
Conduct radiation safety training for staff and encourage safe practices.
Equipment Safety
Verify shielding, warning signs, and safety features; ensure periodic QA testing of X-ray machines.
Radiation Surveys
Perform routine area monitoring and leakage checks.
Incident Reporting
Investigate radiation incidents and report to the licensee and AERB.
Documentation
Maintain records of equipment, dose logs, QA checks, and safety audits.
Support Licensee
Advise and assist the licensee in fulfilling radiation safety obligations.
#10 Facility planning will be discussed in the next presentation
#16 ALARA- stands for as low as reasonably achievable