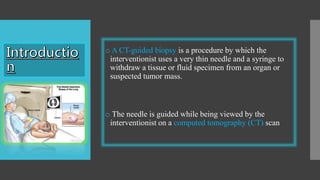
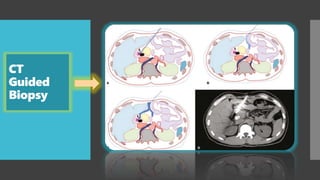
CT-guided biopsy is a minimally invasive procedure to obtain tissue samples from suspicious lesions using a thin needle guided by CT imaging, performed on various organs except the spleen due to bleeding risks. CT enterography is a non-invasive diagnostic technique for small bowel disorders, utilizing oral and intravenous contrast, primarily used to evaluate conditions like Crohn's disease and gastrointestinal bleeding. CT colonography, or virtual colonoscopy, serves as a screening method for colorectal cancer and involves preparation that may include purgatives or fecal tagging.