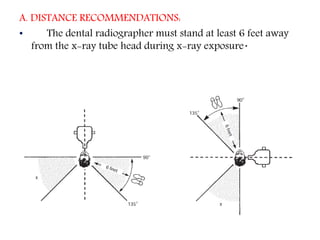
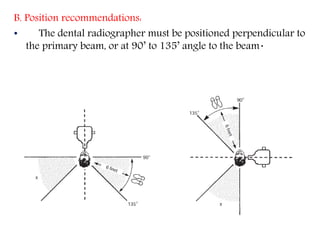
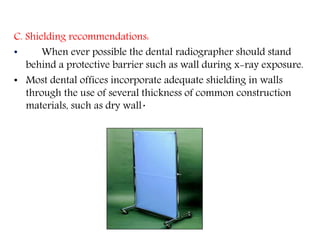
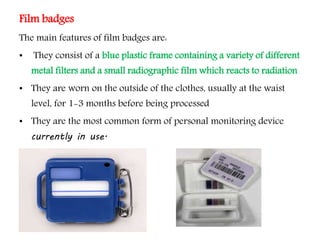
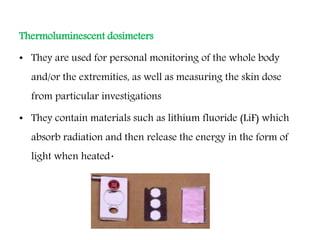
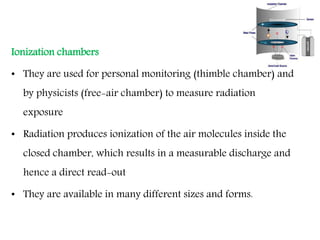
Operator protection when using radiation in dentistry includes following guidelines on distance, position, and shielding from the primary x-ray beam. Distance recommendations state the radiographer should stand at least 6 feet away, while position recommends being perpendicular or at a 90-135 degree angle to the beam. Shielding like protective barriers should also be used when possible. Radiation exposure is monitored through equipment monitoring for leakage radiation and personnel monitoring using film badges, thermoluminescent dosimeters, or ionization chambers. Radiation safety legislation establishes exposure limits for public and occupational exposure to ensure protection of patients, operators, and the environment.