Download to read offline

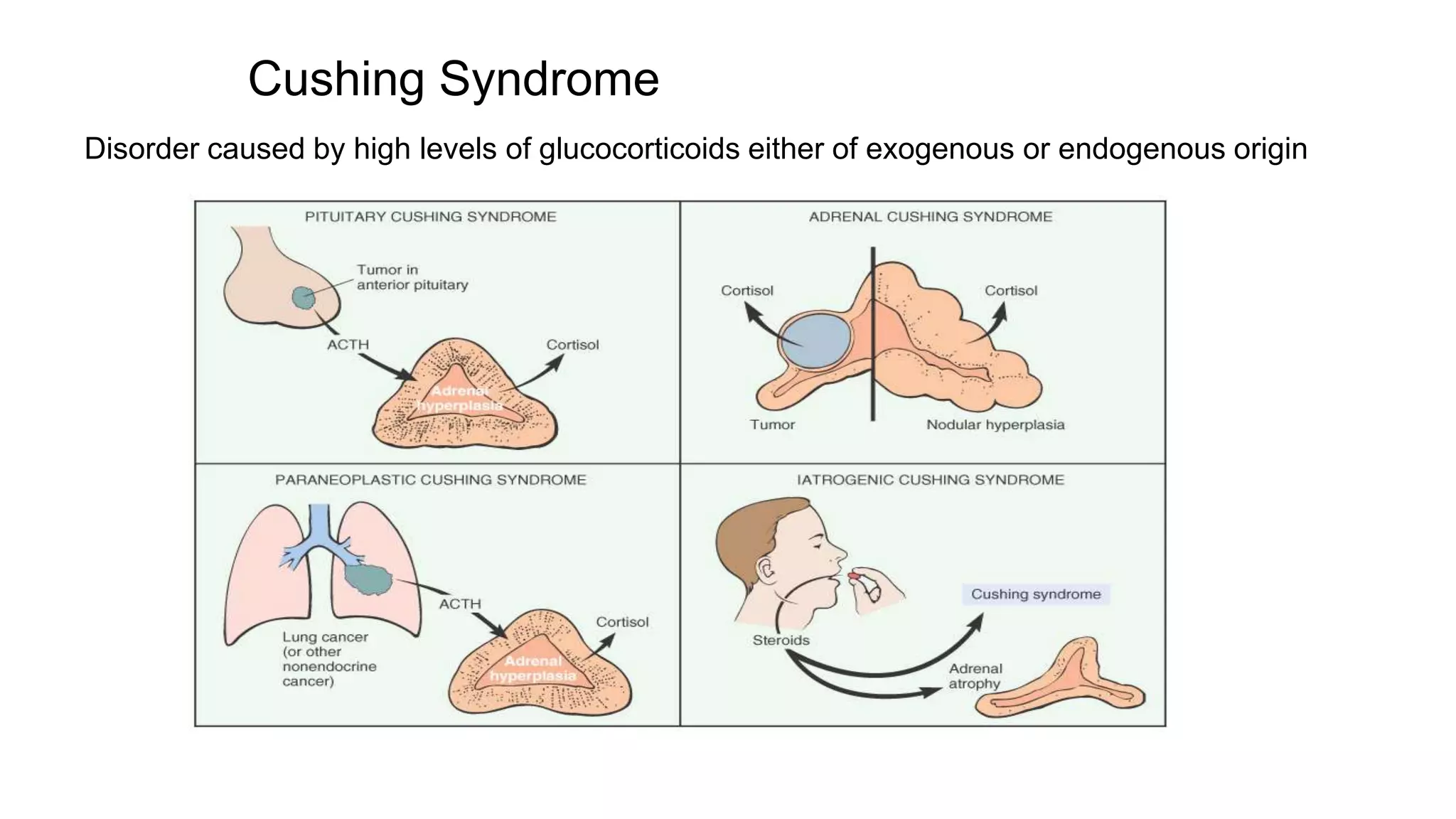
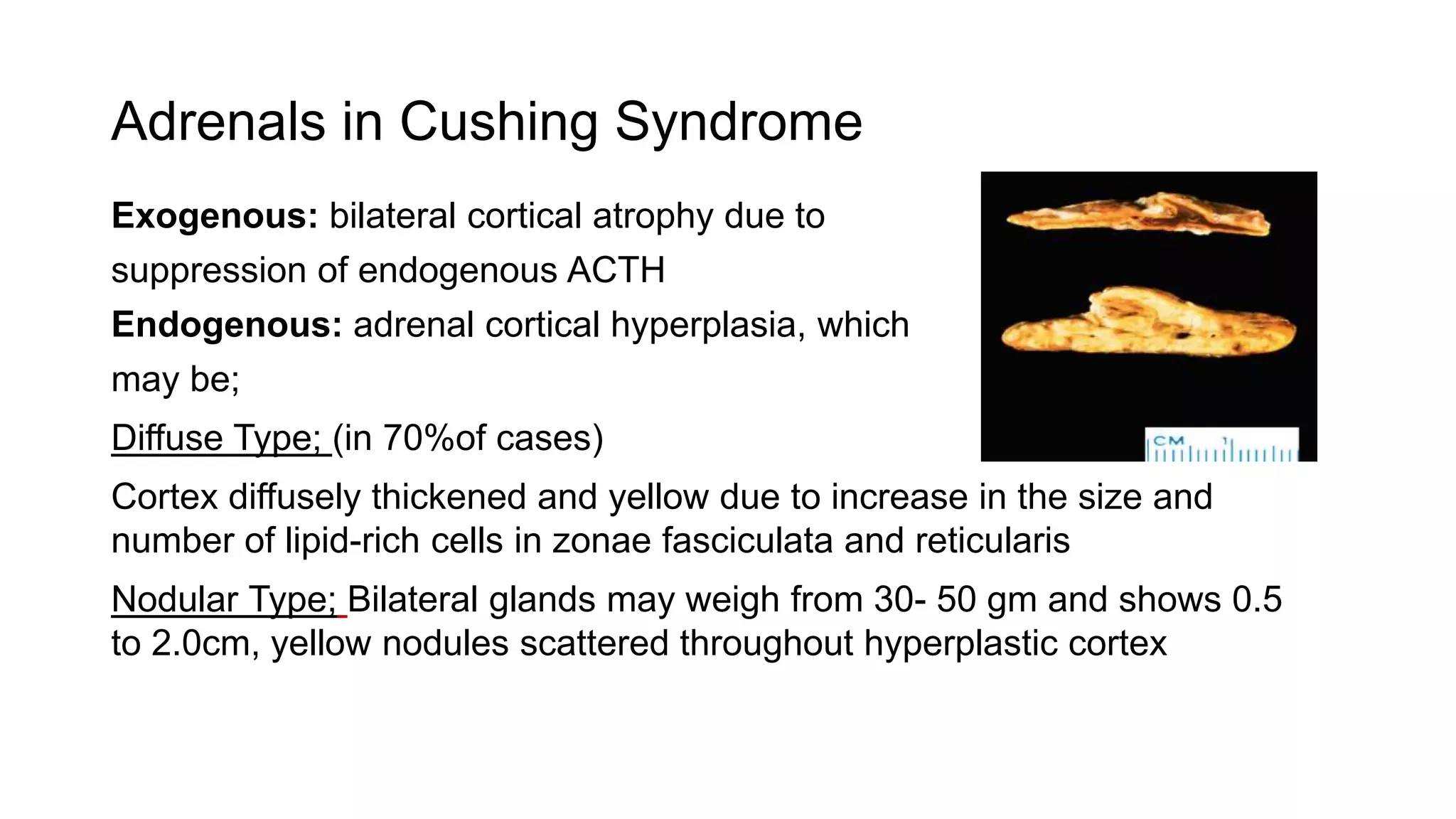
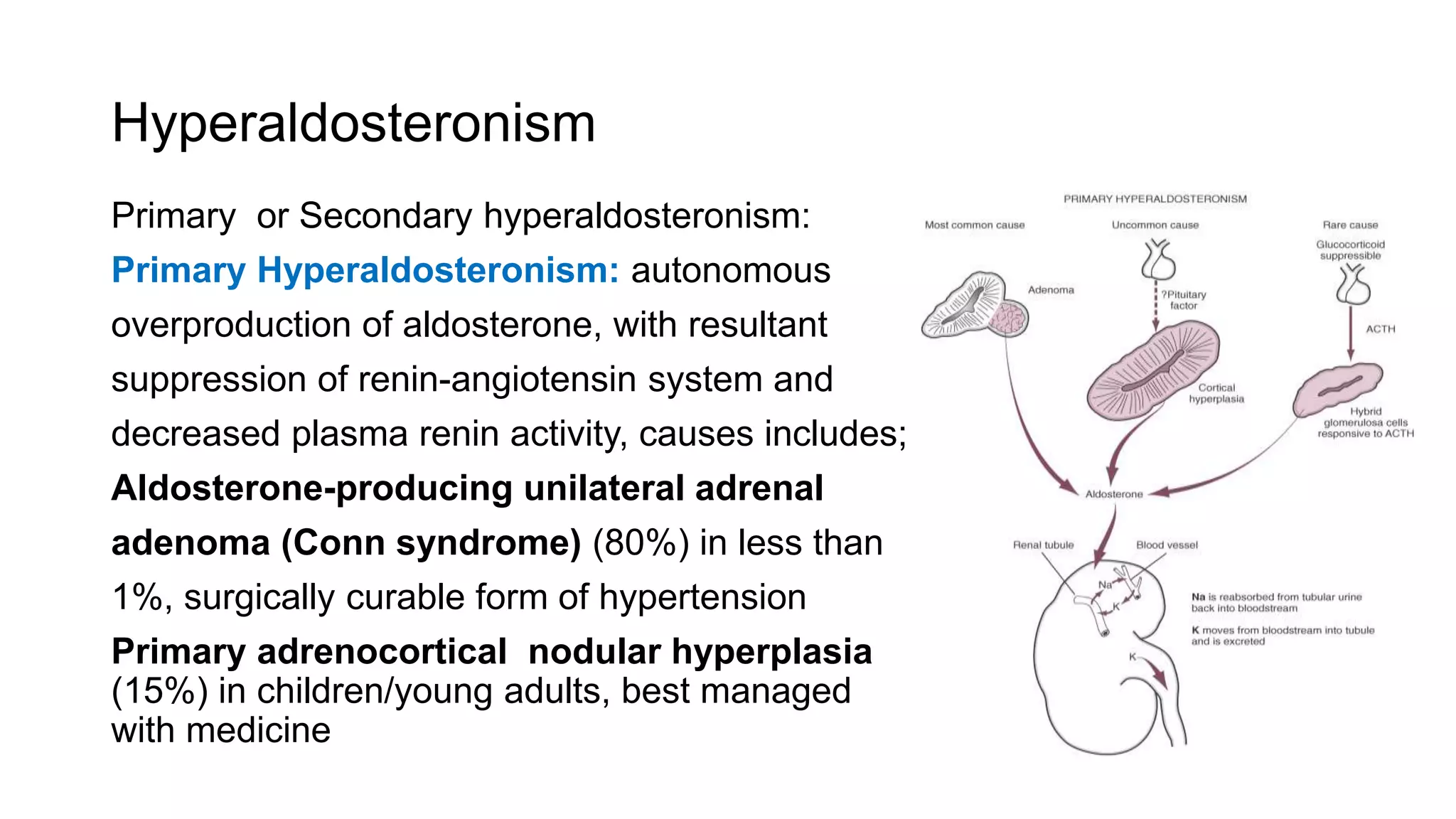





Adrenal cortical disorders can cause hyperfunction or hypofunction of the adrenal cortex. Adrenal cortical hyperfunction includes Cushing syndrome, Conn syndrome (hyperaldosteronism), and adrenogenital syndrome. Cushing syndrome is caused by excessive glucocorticoids and results in adrenal cortical hyperplasia. Conn syndrome is characterized by autonomous overproduction of aldosterone and is commonly caused by an aldosterone-producing adrenal adenoma. Adrenal cortical hypofunction includes primary adrenocortical insufficiency (Addison's disease) and secondary adrenocortical insufficiency caused by decreased ACTH stimulation of the adrenals. Primary adrenocortical insufficiency is often auto























































































