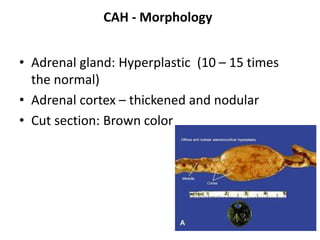
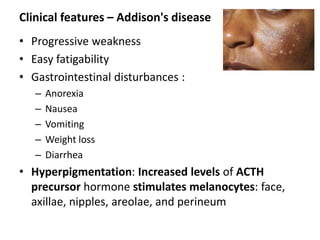
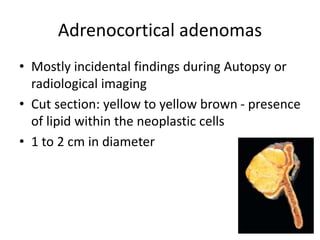
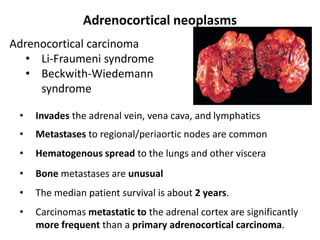
This document discusses various adrenal gland disorders including androgenital syndromes, congenital adrenal hyperplasia, Addison's disease, adrenal adenomas, and adrenocortical carcinoma. Congenital adrenal hyperplasia is described as the most common cause of androgenital syndromes and is usually due to a 21-hydroxylase deficiency which results in masculinization of females. Addison's disease represents chronic adrenal insufficiency and presents with weakness, fatigue, and hyperpigmentation. Adrenocortical carcinomas are aggressive tumors that commonly metastasize to regional lymph nodes and lungs.