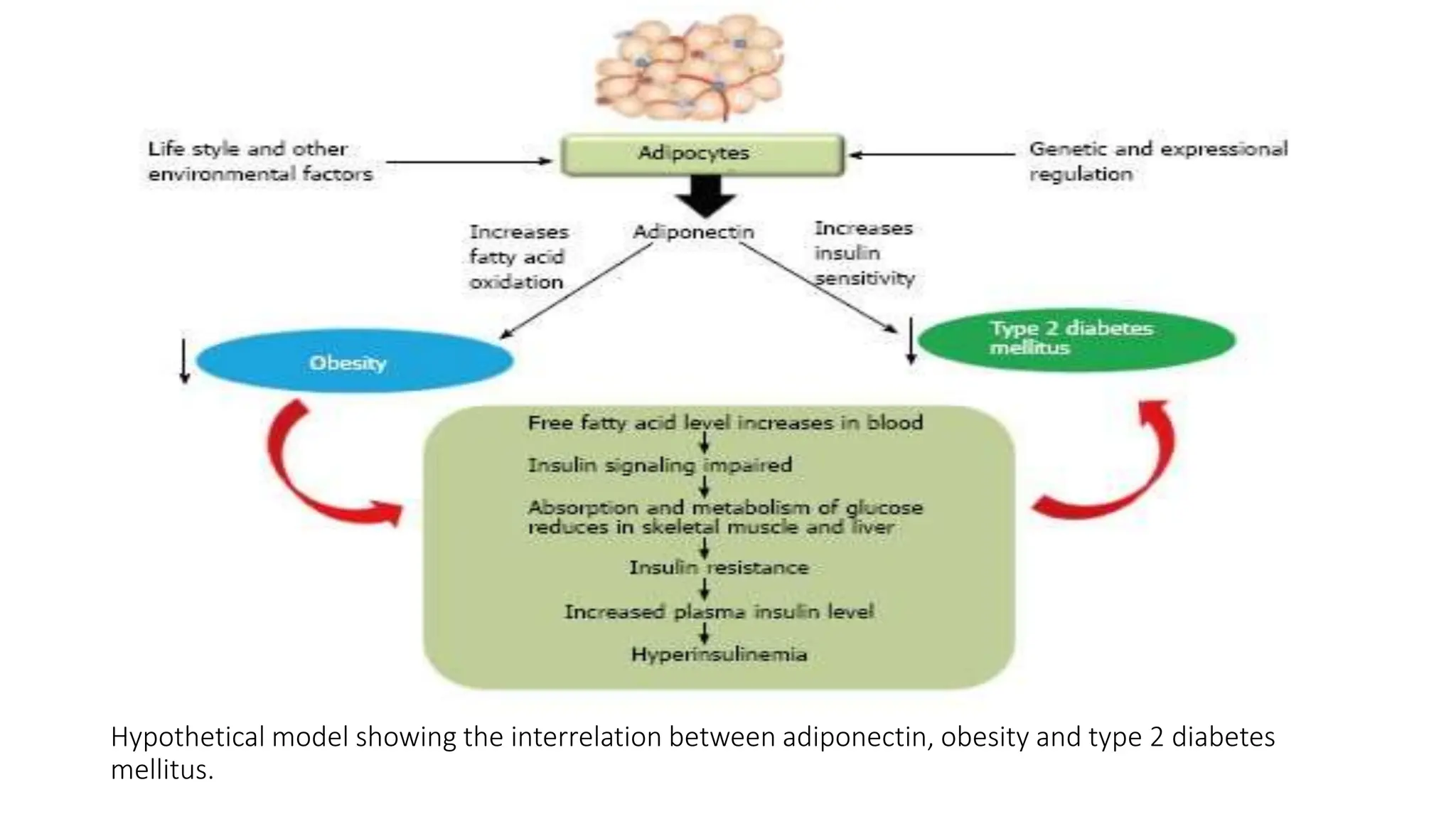
Adiponectin is an adipokine that is decreased in obesity and has anti-diabetic, anti-inflammatory, and cardioprotective effects. It acts through two receptors, AdipoR1 and AdipoR2, and has various actions including increasing insulin sensitivity, fatty acid oxidation, and decreasing inflammation. Low levels of adiponectin are associated with increased risk of metabolic syndrome, hypertension, chronic kidney disease, obstructive sleep apnea syndrome, diabetic retinopathy, cancer, and chronic obstructive pulmonary disease. Enhancing adiponectin expression and activity through lifestyle changes, drugs, recombinant adiponectin, or peptide mimetics may be a therapeutic approach for treating obesity and related