Downloaded 39 times

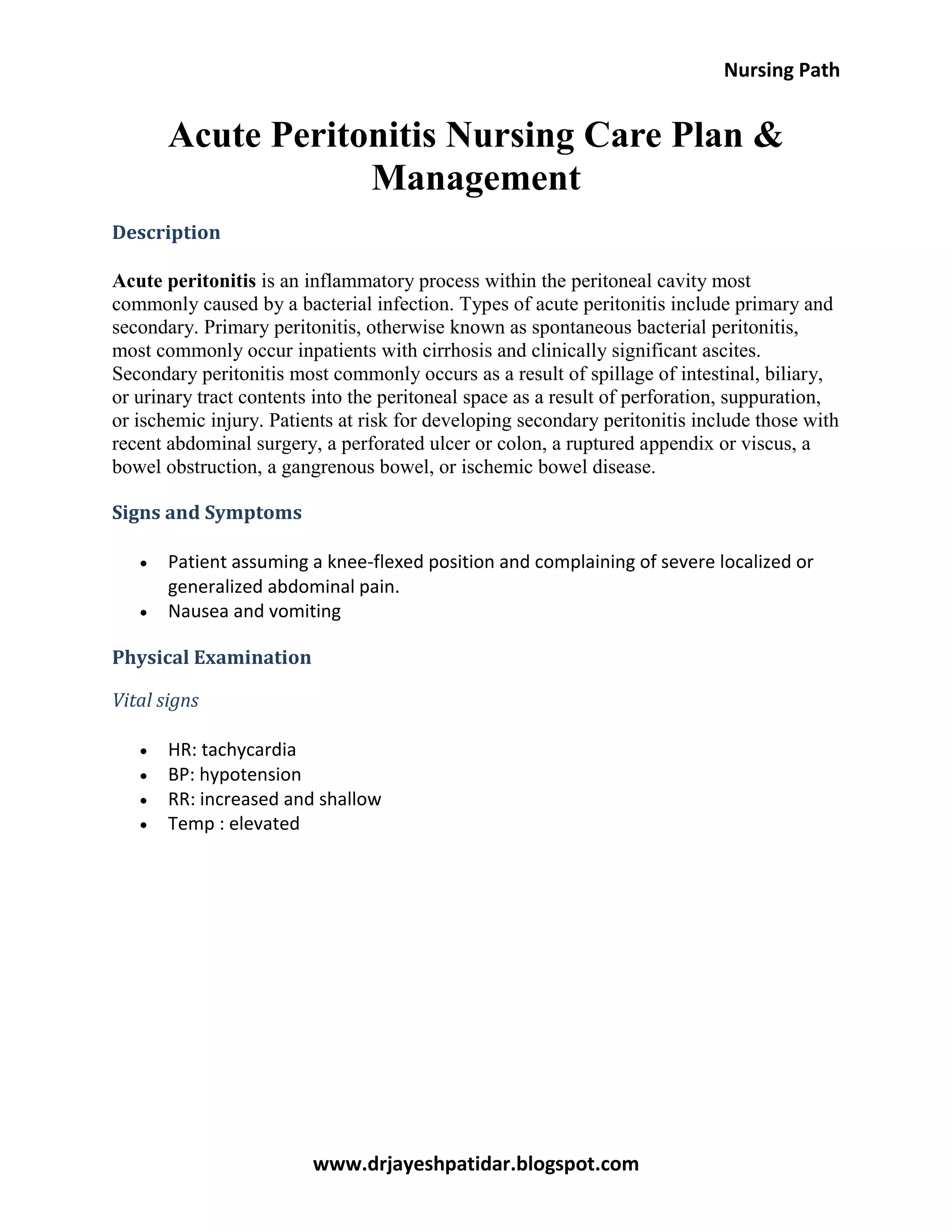



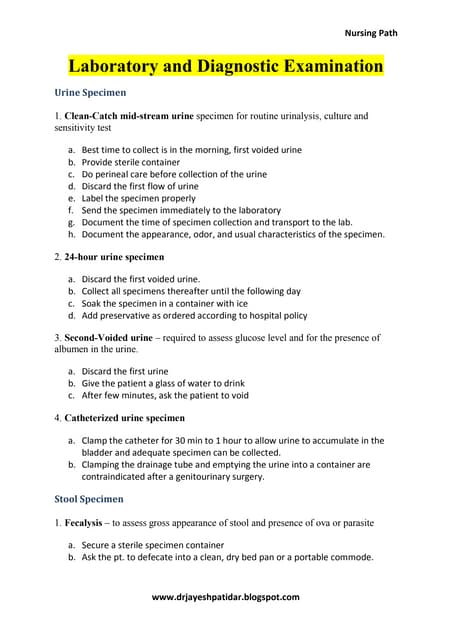
Acute peritonitis is an inflammatory condition of the peritoneal cavity, primarily caused by bacterial infections. It can be classified into primary, often linked to cirrhosis, and secondary peritonitis, which results from various abdominal injuries or infections. Nursing care focuses on monitoring vital signs, fluid balance, and administering treatments like IV fluids and antibiotics while assessing the patient's abdominal condition and overall health.


![Nursing care for patient with CHICKEN POX [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/chickenpoxautosaved-240226082212-b91964d3-thumbnail.jpg?width=640&height=640&fit=bounds)