This document provides an overview of acute pancreatitis including its anatomy, etiology, pathophysiology, diagnosis, severity assessment, treatment, and complications. Some key points:
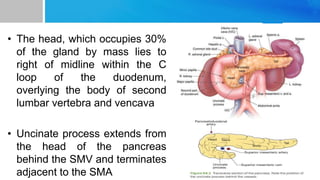
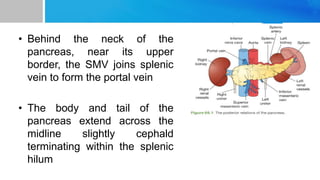
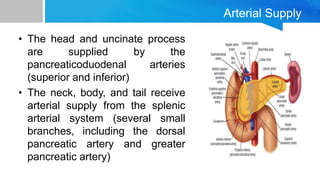
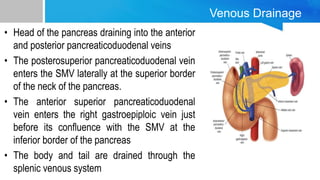
- The pancreas is located in the retroperitoneum and has a head, neck, body and tail supplied by various arteries and veins.
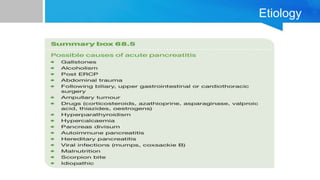
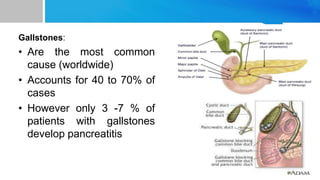
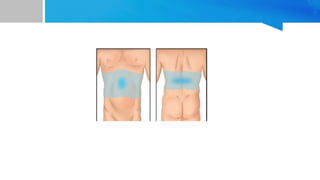
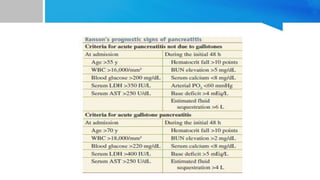
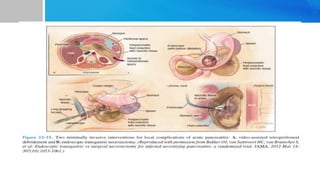
- Acute pancreatitis is defined as inflammation of the pancreas with abdominal pain and elevated pancreatic enzymes. Common causes include gallstones, alcohol use, and hyperlipidemia.
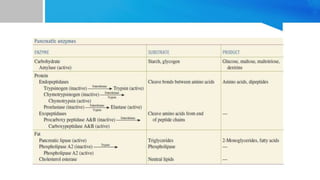
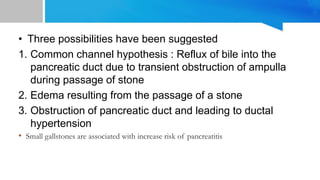
- Inflammation occurs when pancreatic enzymes prematurely activate within the pancreas, causing injury. Systemic complications can develop depending on severity.
- Diagnosis involves history, exam, and lab tests































![Acute pancreatitis [Autosaved].pptx surgery](https://cdn.slidesharecdn.com/ss_thumbnails/acutepancreatitisautosaved-240829144740-b197e85a-thumbnail.jpg?width=640&height=640&fit=bounds)






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



