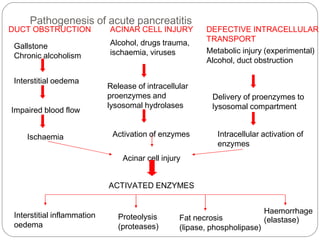
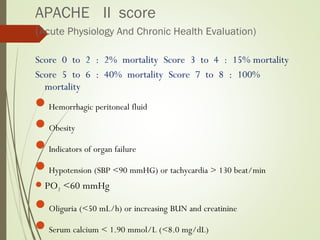
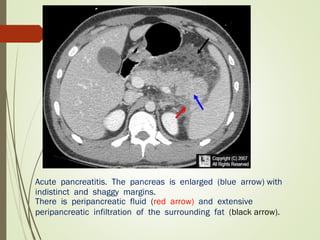
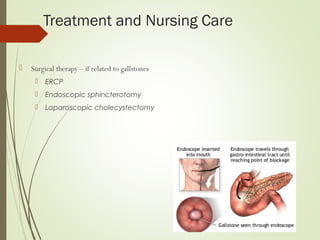
The document discusses acute pancreatitis, defining it as inflammation of the pancreas induced by activation of pancreatic enzymes. It describes the various causes including biliary tract diseases, alcohol use, viral infections, drugs, trauma, and idiopathic causes. Symptoms include severe epigastric pain, nausea, vomiting, and fever. Laboratory tests can show elevated amylase and lipase levels. Treatment focuses on pain relief, fluid resuscitation, suppressing pancreatic enzymes, and treating complications such as pseudocysts and abscesses. Prognosis depends on factors like the Ranson score and presence of organ failure.





























![Alcoholic liver disease [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/alcoholicliverdiseaseautosaved-210106093112-thumbnail.jpg?width=640&height=640&fit=bounds)













![Acute pancreatitis [Autosaved].pptx surgery](https://cdn.slidesharecdn.com/ss_thumbnails/acutepancreatitisautosaved-240829144740-b197e85a-thumbnail.jpg?width=640&height=640&fit=bounds)






















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




