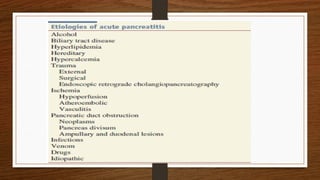
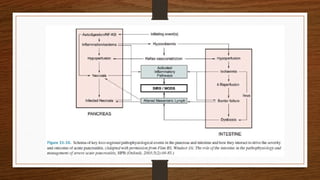
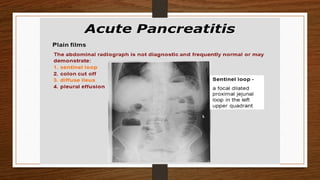
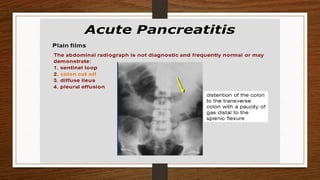
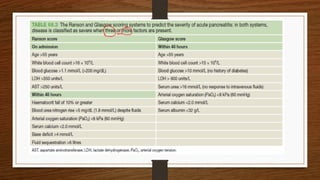
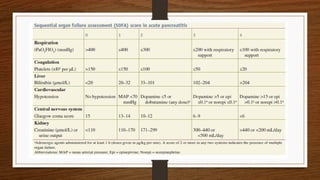
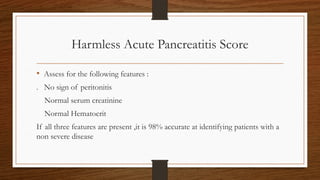
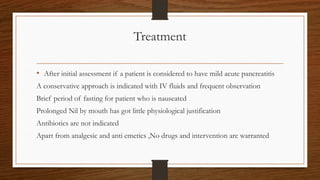
This document focuses on acute pancreatitis, covering its anatomy, physiology, epidemiology, etiology, pathophysiology, diagnosis, treatment, and prognosis. It highlights the conditions and risk factors leading to acute pancreatitis, such as gallstones and alcohol use, and elaborates on diagnostic criteria and treatment approaches for mild and severe cases. Prognosis is assessed using various scoring systems to predict mortality based on clinical features.