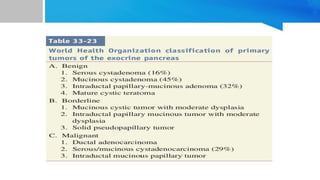
1. Pancreatic cystic neoplasms include serous cystic neoplasms, mucinous cystic neoplasms, and intraductal papillary mucinous neoplasms.
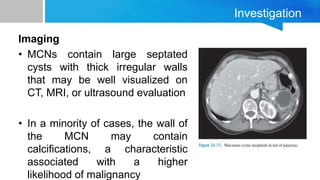
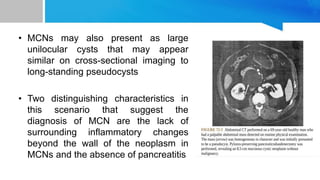
2. Mucinous cystic neoplasms present as large septated cysts more commonly in young women and have thick irregular walls that may contain calcifications. Surgical resection is the treatment of choice.
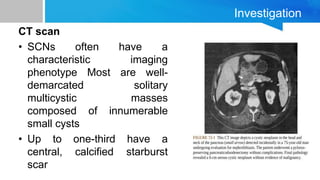
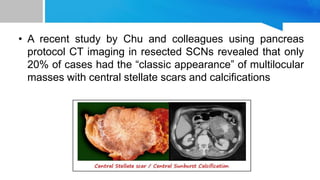
3. Serous cystic neoplasms typically appear as well-circumscribed masses composed of numerous small cysts and have a characteristic honeycomb appearance. They generally have an excellent prognosis with surgical resection reserved for symptomatic cases.