1. Pre-operative preparation begins at initial patient contact and aims to optimize patient outcomes through thorough assessment, medical optimization, risk evaluation, and informed consent.
2. A complete history, physical exam, and relevant lab/imaging investigations are used to evaluate any medical issues and surgical risks. Comorbidities like cardiovascular or respiratory diseases require specialized management.
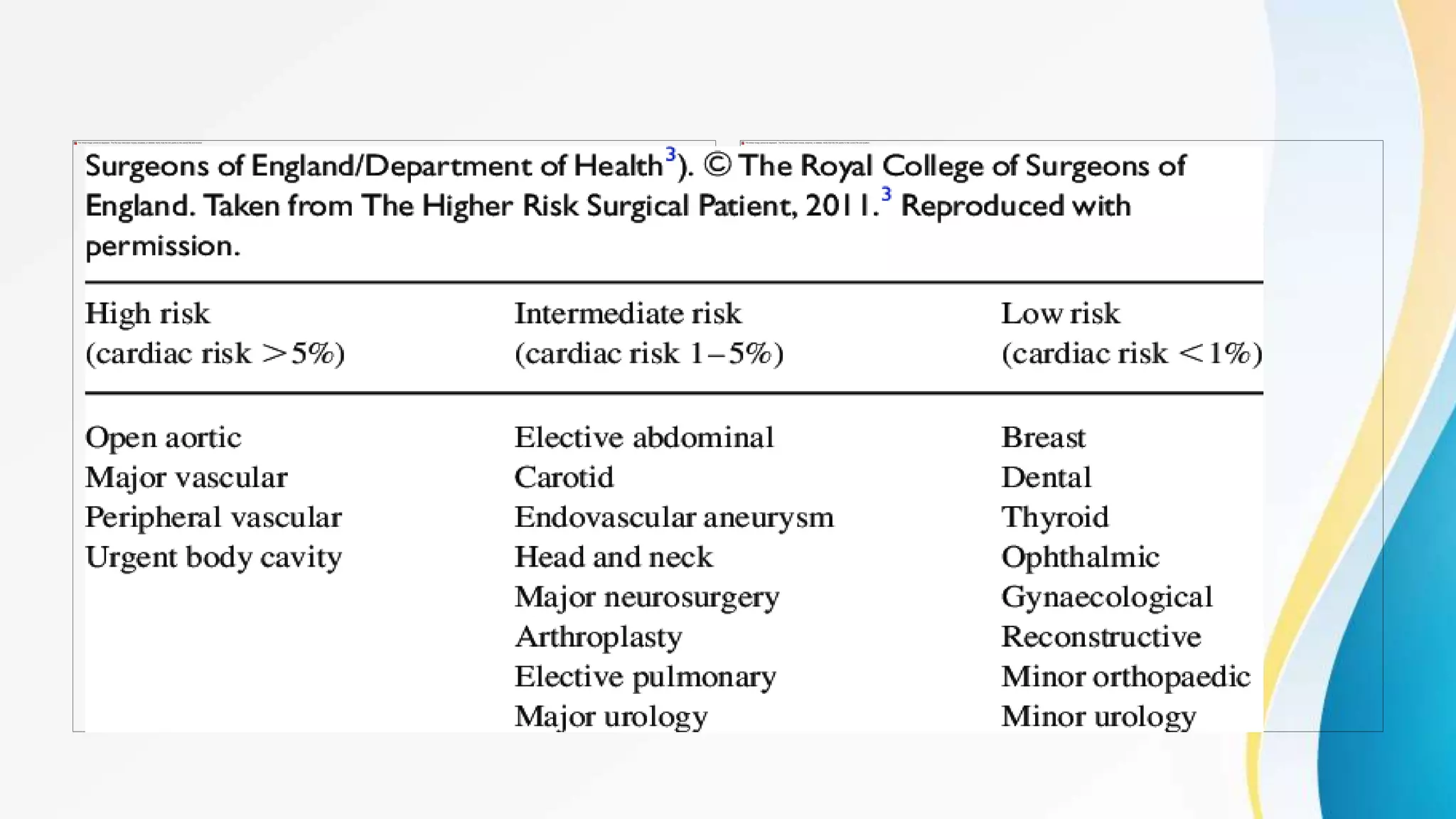
3. High-risk patients undergo detailed optimization, including treating infections, stabilizing medications, and potentially admitting to critical care post-operatively. Proper pre-op skin/hair preparation, antibiotic prophylaxis timing, and elimination help reduce surgical site infections.