ACUTE LIMB ISCHEMIA
Dr.Walid Gamal, MD
Assistant Professor and Head of Vascular Surgery
Department, Qena Faculty Of Medicine
South Valley University
2.
Surgical anatomy
1
-
large arteries:e.g. aorta, they contain
considerable elastic tissue
2
-
medium sized arteries:e.g femoral artery,these posses
less elastic tissue and more
muscle fibers
3
-
small sized arteries:e.g digital arteries,the wall is
primarily of smooth muscle fibers
4
-
Terminal arteries:these are vessels 50-100 microns in
diameter ,their wall is composed of endothelial
lining ,internal elastic lamina and 2 layers of smooth
muscle fibers
.
3.
5- Arterioles: havea diameter of 20-50 microns,they
are similar to terminal arteries but
have only one layer of smooth muscle fibers
•
Ischemia means diminished blood supply(may be
acute or chronic)
The effect of ischemia depends on
:
1
-
type of artery: some arteries have efficient collateral
circulation e.g, subclavian artery while brachial and
popliteal arteries have poor collaterals
4.
2- The rateof occlusion of the artery:Acute
ischemia is much more serious than chronic
ischemia as there is no sufficient time to
collaterals to develop
3- The state of collateral vessels: Healthy
collateral vessel can compensate to some
extent the effect of ischemia
4-The general condition of the patient: The
presence of myocardial insufficiency or sever
anemia will exacerbate the effect of ischemia
Thrombosis
• Secondary toASO: distal SFA, aorta, popliteal
• In absence of stenotic lesion:
– Intra-arterial injections
– hypercoagulable states: e.g. malignancy,
antiphospholipid syndrome, etc..
• Thrombosis of bypass grafts (kinking,
stenosis, anastomotic lesions, ..).
10.
Because the managementis different
Because the management is different
Embolism versus Thrombosis
Embolism
Thrombosis
Sources
Frequently detected
Not specified
Onset
Sudden
Acute
Site
Normal vessels, soft
On top of a stenosis, calcified
Previous complaint
Rare
Symptoms of chronic ischemia
Findings
Normal pulses
Evidence of peripheral arterial
disease
Multiplicity
Multiple sites
Single site
Angiography
No or minimal ASO,
sharp cut off
(Fontaine sign),
multiple cclusions,
no collaterals
Diffuse atherosclerosis, tapered and
irregular cut off, developed
collaterals
11.
Pathophysiology
• Depends on:
–Degree of obstruction (complete or partial)
– Site of occlusion
– Presence of collaterals
– Affected tissues.
• Sluggish circulation distal to the occlusion
secondary thrombosis occlusion of collaterals.
• Different tissues can tolerate ischemia at different
rates (brain and heart versus skin, subcutaneous,
and muscles).
12.
• Nerves: Firstto be affected (irreversible
damage after 6 hours)
• Muscles: more tolerant (up to 6-10 hours).
• Skin: last to show necrosis.
Pathophysiology (Cont.)
13.
• Cellular ischaemia(Revascularization)
– Alteration of cell wall permeability Na+
and
water influx intra and extra cellular edema
compartment syndrome
– Release of K +
hyperkalaemia cardiac arrest.
– Release of myoglobin after muscle infarction
precipitate in renal tubules myoglobinuria and
acute renal failure.
Pathophysiology (Cont.)
14.
Pathophysiology (Cont.)
• Accumulationof acidic products of anaerobic
metablolism metabolic acidosis.
• During reperfusion, oxygen free radicals
accumulate cellular insult and necrosis
(Mannitol and free radical scavengers).
15.
Classifications
• Partial
• Total
•Late
• Viable
• Threatened
– Marginally (reversible with
prompt treatment)
– Immediately (reversible with
immediate treatment)
• Irreversible
16.
Diagnosis
• History: sourceof embolism (e.g. cardiac
patients), risk factors for atherosclerosis.
• Clinical picture: 6 Ps
– Pain (sudden / acute onset, severe, steady, starts
most distal).
– Pallor or cyanosis
– Parasthesia (numbness anaesthesia due to nerve
isch.)
– Pulselessness (sudden loss of previously palpable
pulse = embolic).
– Poikelothermia (cooling of the limb)
– Paralysis (fine movement first due to motor nerve
isch. then because of nerve and muscle).
18.
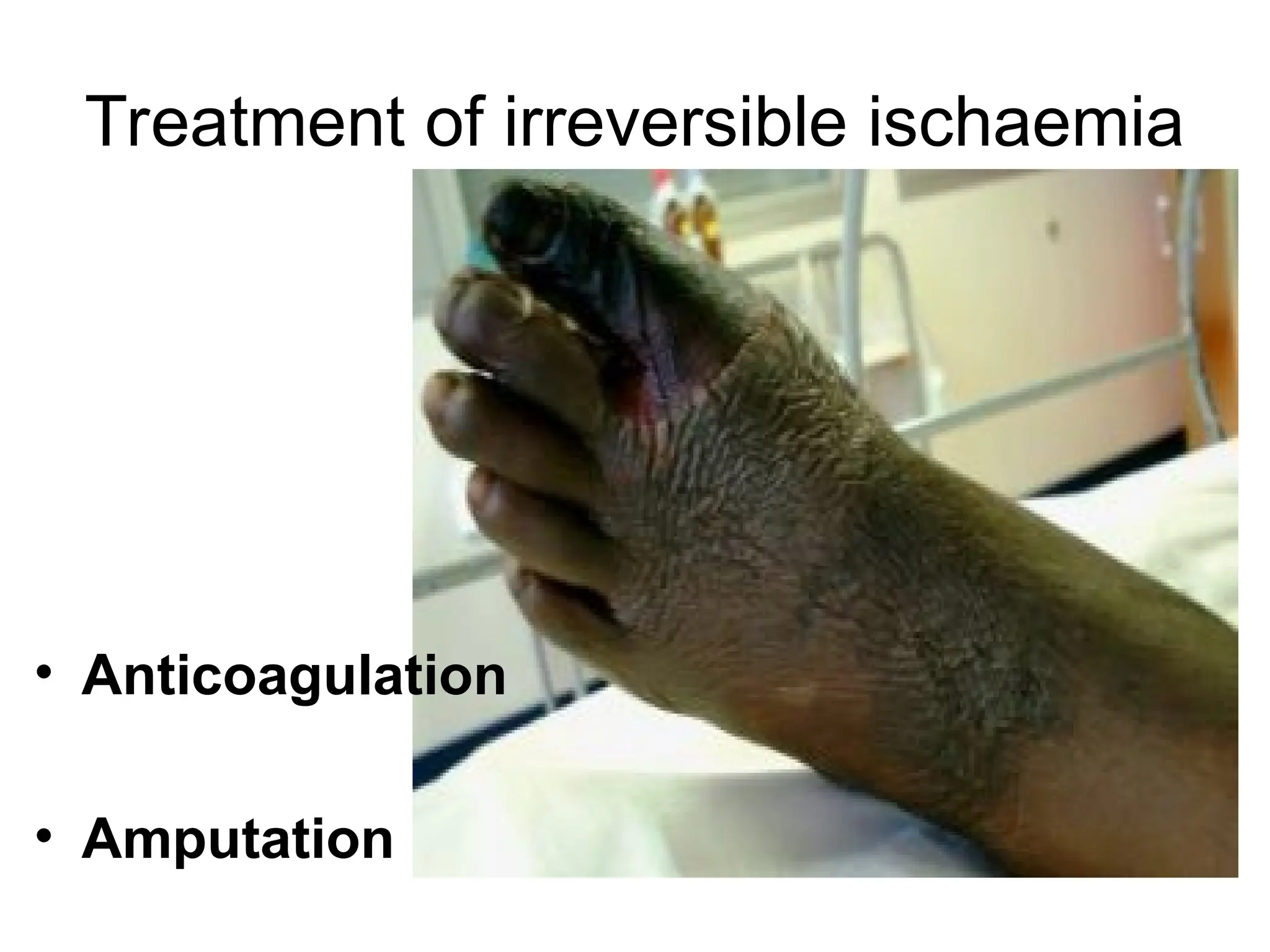
Acute late (irreversible)ischaemia
• Swollen limb
• Tender muscles
• Loss of muscle turgor (doughy).
• Fixed cyanotic color changes, marbling,
necrosis, desquamation.
• Rigor mortis.
24.
Investigations
• Doppler US(to detect blood flow)
– ABI.
– Segmental pressure.
• Imaging:
– Duplex US
– Contrast angiography
• When?
• Why? Site / cause of occlusion (aneurysm,
thrombosis, entrapment, collaterals, dissection,
therapeutic)
If I refuseto allow my leg to be
amputated, its mortification may
prove that I was wrong, but if I let
the leg go, no body can ever prove
that the surgeon was wrong.
Operation is therefore the safe side
for the surgeon.
George Bernard Shaw,
1856-1950
40.
Differential diagnosis
• DVT(swollen limb with difficult pulse
palpation)
• Neurologic disorders: e.g. paraplegia
• Low cardiac output.
• Frost bite and other vasospastic diseases.
• Chronic limb ischaemia.