1) The document describes the surgical techniques for both open and laparoscopic appendectomy.
2) For open appendectomy, the classic McBurney incision is made and layers are separated to expose the appendix which is then ligated and removed.
3) For laparoscopic appendectomy, 3 ports are used to expose the appendix which is then dissected from surrounding tissues, its blood supply ligated, and base stapled before removal.
![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 1
31 APPENDECTOMY
Hung S. Ho, M.D., F.A.C.S.
First depicted in anatomic drawings in 1492 by Leonardo da retracted medially without being divided [see Figure 3].
Vinci, the vermiform appendix was described as an anatomic A foul smell or the presence of pus on entry into the peri-
structure in 1521 by Jacopo Berengari da Carpi, a professor of toneum is an indication of advanced or perforating appendicitis.
human anatomy at Bologna. Appendicitis became recognized as a The free peritoneal fluid is collected for bacteriologic analysis.The
surgical disease when the Harvard University pathologist Reginald appendix is located by following the cecal taeniae distally. The
Heber Fitz read his analysis of 257 cases of perforating inflamma- inflamed appendix usually feels firm and turgid. The appendix,
tion of the appendix and 209 cases of typhlitis or perityphlitis at together with the cecum, is delivered into the surgical incision and
the 1886 meeting of the Association of American Physicians. In held with a Babcock tissue forceps. If this step proves difficult, the
this landmark report, Fitz correctly pointed out that the frequent appendix can sometimes be swept into the field with the surgeon’s
abscesses in the right iliac fossa were often due to perforation of right index finger as gentle traction is maintained on the cecum
the vermiform appendix, and he referred to the condition as with a small, moist gauze pad held in the left hand [see Figure 4].
appendicitis.1 Among his classic observations of the disease was Care should be taken at this point not to avulse the friable and
his emphasis on the “vital importance of early recognition” and its possibly necrotic appendix. To deliver a retrocecal appendix, it
“eventual treatment by laparotomy.” It was not until 1894 that may be necessary to mobilize the ascending colon partially by
Charles McBurney first described the surgical incision that bears dividing the peritoneum on its lateral side, starting from the termi-
his name and the technique of appendectomy that was to become nal ileum and proceeding toward the hepatic flexure.
the gold standard for appendectomy throughout the 20th century The mesoappendix, containing the appendicular artery, is
and into the 21st.2 divided between clamps and ligated with 3-0 absorbable sutures
Although appendectomy has traditionally been done—and [see Figure 5]. The appendix is held up with a Babcock tissue for-
largely continues to be done—as an open procedure, there has ceps, and its base is crushed with a straight mosquito arterial for-
been increasing interest in laparoscopic appendectomy since the ceps.The mosquito forceps is then opened, moved up the appen-
beginning of the 1990s. At present, however, the only patients for dix, and closed again. The base of the appendix is doubly ligated
whom laparoscopic appendectomy appears to offer significant with 2-0 absorbable sutures at the point where it was crushed, so
advantages are women of childbearing age, obese patients, and that a cuff of about 3 mm is left between the forceps and the tie.
patients with an unclear diagnosis [see Figure 1]. Accordingly, the The appendix is divided by running a scalpel along the under-
gold standard for surgical treatment of acute appendicitis remains side of the forceps.The mucosa of the appendiceal stump is fulgu-
open appendectomy as described by McBurney. The occasional rated with the electrocautery. The stump is not routinely invagi-
patient with chronic appendicitis should be electively treated with nated into the cecum. In those rare cases in which the viability of
the laparoscopic approach. the appendiceal base is in question, a 2-0 absorbable purse-string
suture is placed in the cecum, and the stump is invaginated as the
suture is tied; if this is done, palpation for a patent ileocecal valve
Operative Technique is indicated.The operative field is then checked for hemostasis. In
cases of perforating appendicitis, the right paracolic gutter and
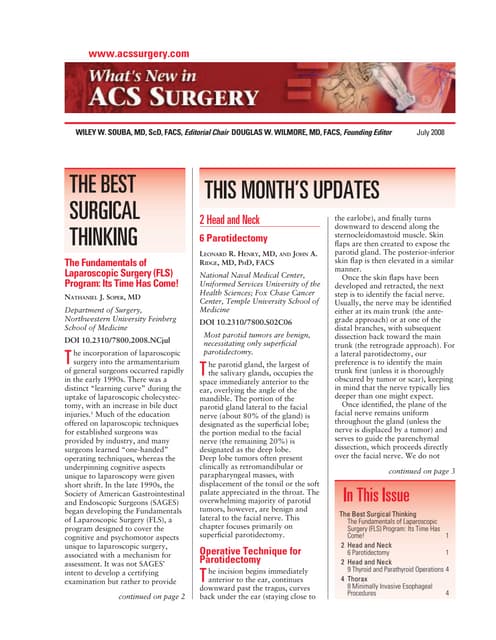
OPEN APPENDECTOMY
pelvis are irrigated and thoroughly aspirated to ensure that any
With the patient in the supine position, general anesthesia is collected pus or particulate material is removed.
induced and the abdomen is prepared and draped in a sterile fash- The peritoneum is then closed with a continuous 3-0
ion so as to expose the right lower quadrant. The skin incision is absorbable suture.The fibers of the transversus abdominis and the
made in an oblique direction, crossing a line drawn between the internal oblique muscle fall together readily, and their closure can
anterior superior iliac spine and the umbilicus at nearly a right be completed with two interrupted 3-0 absorbable ligatures. The
angle at a point about 2 to 3 cm from the iliac spine. This point, external oblique aponeurosis is closed from end to end with a con-
McBurney’s point, is approximately one third of the way from the tinuous 2-0 absorbable suture. Scarpa’s fascia is approximated
iliac spine to the umbilicus [see Figure 2]. The subcutaneous fat with interrupted 3-0 absorbable sutures, and the skin is closed
and fascia are incised to expose the external oblique aponeurosis. with a continuous subcuticular 4-0 absorbable suture and rein-
A slightly shorter incision is made in this aponeurosis; first, a forcing tapes (Steri-Strips).
scalpel is used, and then, the incision is extended with scissors in If the wound has been grossly contaminated, the fascia and
the direction of the fibers of the muscle and its tendon in such a muscles are closed as described, but the skin is loosely approxi-
way that the fibers are separated but not cut. mated with Steri-Strips, which can easily be removed after the
The fibers of the internal oblique muscle and the transver- procedure if surgical site infection or abscess develops. An alterna-
sus abdominis are separated with a blunt instrument at nearly tive approach is to leave the skin and the subcutaneous tissue open
a right angle to the incision on the external oblique aponeuro- but dressed with sterile nonadherent material and then to perform
sis. The parietal peritoneum is lifted up, with care taken not to delayed primary closure with Steri-Strips on postoperative day 4
include the underlying viscera, and is opened in a transverse or 5. A meta-analysis of 27 studies involving 2,532 patients with
fashion with a scalpel.This incision is then enlarged transverse- gangrenous or perforating appendicitis concluded that the risk of
ly with scissors. When greater exposure is required, the lateral surgical site infection was no higher with primary closure than
edge of the rectus sheath is incised and the rectus abdominis with delayed primary closure.3](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-1-320.jpg)
![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 2
Patient has clinically suspected acute appendicitis
Obtain history.
Perform physical examination.
Typical signs and symptoms Atypical signs and symptoms are present
are present
Perform additional procedure(s) to confirm
diagnosis.
Patient is not obese Patient is obese or is a
and is not a woman woman of childbearing
of childbearing age age Ultrasonography or
CT scanning Diagnostic laparoscopy
Perform open Perform laparoscopic
appendectomy. appendectomy.
Diagnosis is Other pathologic
Diagnosis is Diagnosis is confirmed condition is
confirmed not confirmed identified
Perform
Perform Treat other pathologic
laparoscopic
appendectomy. condition(s).
appendectomy.
Figure 1 Shown is an algorithm Imaging study identifies Results of imaging
Results of imaging study
for choosing between treatment are completely normal other pathologic condition study are equivocal
options for patients with suspected
acute appendicitis. Discharge patient. Treat other pathologic Perform diagnostic
condition(s). laparoscopy (see above).
LAPAROSCOPIC APPENDECTOMY
The patient is placed in the supine position, with both arms
tucked along the sides, and general anesthesia is induced. De-
compression with an orogastric tube should be routine, as should
placement of a urinary Foley catheter and use of lower-extremity
sequential compression devices.The surgeon should stand on the
patient’s left side, with the assistant (who operates the camera)
near the patient’s left shoulder [see Figure 6]. The monitors are
placed on the opposite side of the operating table so that both the
surgeon and the assistant can view the procedure at all times.
The abdomen is prepared and draped in a sterile fashion so as
to expose the entire abdomen. A three-port approach is routinely
used [see Figure 6]. All skin incisions along the midline are made
vertically to allow a more cosmetically acceptable conversion to
laparotomy, should this become necessary. The suprapubic port Linea Alba
must be large enough to accommodate the laparoscopic stapler
(usually 12 mm); the other two ports can be smaller (e.g., 5 or 10
2
mm).The ports are placed as far away from the operative field as /3
possible to permit the application of a two-handed dissection
technique. The use of a 30° angled scope facilitates operative view- 1
ing and dissection. /3
With the patient pharmacologically relaxed and in the
Trendelenburg position, a Veress needle is inserted into the peri-
toneal cavity at the base of the umbilical ligament. Aspiration and
Anterior Superior
the saline-drop test are performed to ensure that the tip of the Iliac Spine
needle is correctly positioned. Pneumoperitoneum is established
by insufflating CO2 to an intra-abdominal pressure of 14 mm Hg.
The first port is placed at the infraumbilical skin incision, the Figure 2 Open appendectomy. Shown are McBurney’s point and
laparoscope is inserted, and a complete diagnostic laparoscopy is McBurney’s incision.](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-2-320.jpg)
![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 3
a b
Rectus Sheath
Internal Oblique
Muscle
External Oblique
Aponeurosis
Internal Oblique
Muscle
Rectus Rectus
Abdominis Abdominis
c Muscle d Muscle
Peritoneum and
Transversalis
Fascia
Internal
Oblique
Injected Peritoneum Internal Oblique
Muscle Muscle
Figure 3 Open appendectomy. Depicted is exposure of the abdominal cavity. The external oblique aponeu-
rosis is opened (a). The fibers of the internal oblique muscle are separated bluntly (b). The parietal peri-
toneum is exposed (c) and opened transversely (d).
performed. Once the diagnosis of acute appendicitis is confirmed The tip of the appendix is grasped and retracted anteriorly
by inspection, the two remaining ports are placed under direct toward the anterior abdominal wall and slightly toward the pelvis;
vision. In many cases, however, the diagnosis cannot be confirmed the mesoappendix is thus exposed in a triangular fashion. A win-
without first placing the second and third ports and exposing the dow between the base of the appendix and the blood supply is cre-
appendix. If purulent fluid is encountered, it should be carefully ated with a curved dissecting forceps.The mesoappendix is divid-
aspirated dry without irrigation to ensure that the infected fluid is ed either with hemostatic clips and scissors or with a laparoscopic
not disseminated throughout the abdominal cavity. gastrointestinal anastomosis (GIA) stapler loaded with a vascular
The appendix is exposed and traced to its base on the cecum by cartridge [see Figure 7]. If a window on the mesoappendix cannot
using an atraumatic retracting forceps. In cases of retrocecal be safely created because of intense inflammation, antegrade dis-
appendix or severe appendiceal inflammation, it is best first to section of the blood supply is necessary.The ultrasonic scalpel is a
mobilize the cecum completely by taking the lateral reflection of handy (albeit expensive) instrument for this purpose. Endoscopic
the peritoneum around the terminal ileum and up the ascending hemostatic clips usually suffice to control the small branches of the
colon with an ultrasonic scalpel (e.g., the Harmonic Scalpel; Ethicon appendicular artery during the course of this dissection.
Endo-Surgery, Inc., Cincinnati, Ohio). Surrounding structures, such The base of the appendix is then cleared circumferentially of any
as the iliac and gonadal vessels and the ureter, should be clearly adipose or connective tissue and is divided with a laparoscopic GIA
identified to minimize the risk of injury. Dissection of the appen- stapler loaded with an intestinal cartridge [see Figure 8]. To ensure
dix can then begin. an adequate closure away from the inflamed appendiceal wall, a](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-3-320.jpg)

![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 5
Camera Operator/ 8% to 41%.5-14 Nonetheless, appendectomy relieves symptoms in
Assistant the vast majority of these patients. When extensive sectioning is
done on histologically normal specimens, it often happens that a
focus of inflammation is found in only a few serial sections. This
condition is known as focal appendicitis—so called because the
polymorphonuclear infiltration is confined to a single focus, while
the remaining appendix is devoid of any polymorphonuclear
cells.15 It is not clear that all cases of acute appendicitis arise from
this focal inflammation; however, such inflammatory foci may be
(10 mm Port)
(5 mm Port) a
(12 mm Port)
Monitor
Surgeon
Figure 6 Laparoscopic appendectomy. Shown are the positioning
and placement of the operative ports, as well as the recommended
positions for the surgeon, the camera operator, and the video
monitor.
small portion of the cecum may have to be included within the sta-
pler. To ensure proper placement of the stapler and to prevent
injury to the right ureter or the adjacent small bowel, the tips of the
stapler must be clearly visualized before the instrument is closed.
The use of an angled scope and an articulated rotating laparoscop-
ic GIA stapler (e.g., Roticulator;AutoSuture, Norwalk, Connecticut)
will facilitate this maneuver. A noninflamed or minimally inflamed
appendix can be ligated with sutures, as described earlier [see Open
Appendectomy, above].The appendix is removed from the abdom-
b
inal cavity, with care taken to avoid direct contact with the abdom-
inal wall. A mildly inflamed appendix can be delivered through one
of the larger ports; a severely inflamed appendix is often too big and
hence should be delivered in a specimen retrieval bag [see Figure 9].
The operative field is irrigated and aspirated dry. Hemostasis is
confirmed, and the cecum is inspected to ensure proper closure of
the appendiceal stump.The ports are removed under direct vision,
the absence of back-bleeding from the port sites is confirmed, and
the abdomen is completely decompressed. All fascial defects larg-
er than 5 mm are closed with 0 absorbable sutures.The skin inci-
sions are reapproximated with a subcuticular 4-0 absorbable
suture and reinforcing Steri-Strips.
Special Considerations
HISTOLOGICALLY NORMAL APPENDIX
Acute appendicitis is the most common cause of an acute sur-
gical abdomen in the United States, and it remains one of the
most challenging diagnoses to make in the emergency depart-
ment. Although the use of advanced diagnostic imaging modalities
(e.g., ultrasonography and computed tomography) has led to
more accurate diagnosis of acute appendicitis in research settings,
it has not been shown to reduce the rate of misdiagnosis of acute
appendicitis in the general population.4 Figure 7 Laparoscopic appendectomy. The mesoappendix is
The incidence of histologically normal appendix in patients divided either with a laparoscopic GIA stapler (a) or with hemo-
with clinical signs and symptoms of acute appendicitis ranges from static clips and scissors (b).](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-5-320.jpg)
![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 6
a b
Figure 8 Laparoscopic appendecto-
my. The mesoappendix having been
divided (a), the base of the appendix
is cleared circumferentially and
divided with a GIA stapler (b).
the earliest recognizable manifestations of appendicitis in some so- a
called negative appendectomies. Furthermore, a substantial pro-
portion of histologically normal appendices removed from patients
with clinical signs and symptoms of acute appendicitis exhibit sig-
nificantly increased expression of tumor necrosis factor–α and
interleukin-2 messenger RNA (a sensitive marker of inflammation
in appendicitis) in germinal centers, the submucosa, and the lam-
ina propria.16 Therefore, appendectomy is recommended in
patients with clinically suspected acute appendicitis even when the
appendix does not appear inflamed during exploration.17
Laparoscopic appendectomy has not been shown to reduce the
incidence of negative exploration in patients with clinically sus-
pected acute appendicitis [see Complications and Outcome Eval-
uation, Open versus Laparoscopic Appendectomy, below].
APPENDICEAL NEOPLASM
b
Neoplastic lesions of the appendix are found in as many as 5%
of specimens obtained with routine appendectomy for acute
appendicitis.18-21 Most are benign. Preoperative detection of such
conditions is rare, and intraoperative diagnosis is made in fewer
than 50% of cases. Appendectomy alone may be curative for
appendiceal mucocele, localized pseudomyxoma peritonei, most
appendiceal carcinoids, and other benign tumors. Definitive man-
agement of an appendiceal mass unexpectedly encountered during
exploration for clinically suspected acute appendicitis depends on
whether the tumor is carcinoid, its size and location, the presence
or absence of metastatic disease, and histologic and immunohisto-
chemical findings [see Figure 10].
Benign neoplasms of the appendix include mucosal hyperplasia
or metaplasia, leiomyomas, neuromas, lipomas, angiomas, and
other rare lesions. Appendiceal adenomas tend to be diffuse and to
have a predominant villous character. Mucus-producing cystade- Figure 9 Laparoscopic appendectomy. The specimen is deliv-
nomas predispose to appendiceal mucocele, sometimes accompa- ered either through one of the larger ports (a) or in a specimen
nied by localized pseudomyxoma peritonei. These lesions are retrieval bag (b).](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-6-320.jpg)
![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 7
rarely symptomatic and are often encountered incidentally during Appendiceal mass is encountered
operation; however, they may also be clinically manifested as acute during exploration for clinically
appendicitis, torsion, intussusception, ureteral obstruction, or suspected acute appendicitis
another acute condition. If the base of the appendix is free of dis-
Determine whether tumor
ease, appendectomy alone is sufficient treatment.
is carcinoid.
Malignant tumors of the appendix primarily consist of carci-
noids and adenocarcinomas; all together, they account for 0.5%
of all GI malignancies.22 The incidence of malignancy in the
appendix is 1.35%.18 Metastasis to the appendix is rare. Carci- Tumor is carcinoid Tumor is
noids are substantially more common than adenocarcinomas in the noncarcinoid
appendix: as many as 80% of all appendiceal masses are carcinoid Assess tumor size and
tumors. Overall, carcinoid tumors are found in 0.5% of all ap- location, and look for Perform immediate
metastases. right hemicolectomy.
pendiceal specimens, and appendiceal carcinoid tumors account
for 18.9% of all carcinoid lesions.23 These tumors are predo-
minantly of neural cellular origin and have a better prognosis than
all other intestinal carcinoid tumors, which typically are of muco- Tumor is > 2 cm, Tumor is < 2 cm,
sal cellular origin. If the tumor is less than 2 cm in diameter, is is located in base is located in body
located within the body or the tip of the appendix, and has not of appendix, or or tip of appendix,
metastasized, appendectomy is the treatment of choice. If the has metastasized and has not
metastasized
lesion is at the base of the appendix, is larger than 2 cm in diam- Perform immediate
eter, or has metastasized, right hemicolectomy [see 5:34 Segmental right hemicolectomy. Perform
Colon Resection] is indicated. In addition, secondary right hemi- appendectomy.
colectomy is indicated if the tumor is invasive, if mucin produc- Initiate histologic and
tion is noted, or if the tumor is found to be of mucosal cellular ori- immunohistochemical
gin at final pathologic examination.24,25 Patients with metastatic Liver metastasis No liver studies.
appendiceal carcinoid tumors appear to have a far better progno- is present metastasis
sis than those with other types of metastatic cancers.24 Therefore, is present
hepatic debulking for symptomatic control is indicated and justi- Perform hepatic
debulking. Observe patient.
fied in cases of liver metastasis.
Primary adenocarcinoma of the appendix is rare, and as yet
there is no firm consensus regarding prognosis, treatment of
choice, and outcome.26 Currently, the recommended treatment is Tumor is invasive, Tumor is not invasive,
right hemicolectomy: a 1993 study found that this approach result- or mucin production and no mucin production
ed in an overall 5-year survival rate of 68%, compared with a rate is noted is noted
of 20% when appendectomy alone was performed.25 The progno-
Perform elective right
sis is determined by the degree of tumor differentiation and by the
hemicolectomy.
histologic stage. As many as one third of these patients have a sec-
ond primary neoplasm, which will be located within the GI tract Tumor is of Tumor is of
about half the time. mucosal origin neural origin
Finally, nonepithelial appendiceal tumors, though extremely Perform Observe patient.
rare, occur as well. Such lesions include malignant and Burkitt elective right
lymphomas, smooth muscle tumors, granular cell tumors, gan- hemicolectomy.
glioneuromas, and Kaposi sarcoma.
Figure 10 Shown is an algorithm for the management of an
INFLAMMATORY BOWEL DISEASE appendiceal mass encountered during exploration for clinically
The appendix is frequently involved in Crohn disease and suspected acute appendicitis.
ulcerative colitis (25% and 50% of cases, respectively), but isolat-
ed Crohn disease of the appendix is rare.27-30 When a histologi-
cally normal appendix is encountered in a patient with active gical exploration. In such cases, diagnostic laparoscopy provides an
Crohn disease, appendectomy should be performed because of excellent view of the pelvic organs, and it offers the potential for
the high risk of recurrent right lower quadrant pain, fever, and easy continuation on to laparoscopic treatment. Ovarian cysts
tenderness. Although isolated Crohn disease of the appendix found in premenopausal women include unilocular clear fluid
may present as acute appendicitis, it is not clear that this condi- cysts (e.g., follicular cysts and corpus luteum cysts), dermoid cysts,
tion will necessarily develop into a more extensive form of Crohn and endometrial cysts.They can be removed by making an incision
disease. Appendectomy is safe in such cases because fistulas on the ovary and separating the cyst from the ovarian cortex.
almost never develop after appendectomy in patients with isolat- Dermoid cysts should be removed in toto to prevent chemical peri-
ed involvement of the appendix. tonitis. Endometrial cysts are best evaporated with the laser: com-
plete removal is very difficult and sometimes impossible.Torsion of
GYNECOLOGIC CONDITIONS the fallopian tube or the ovary can be reversed by gentle detorsion
It is clear that the presentation of right lower quadrant pain in a of the organ with atraumatic forceps. If there is no evidence of
woman remains a challenge to the treating physician. Frequently, ischemia, no further therapy is indicated. If there is gangrene with
the causes can be identified by means of proper blood work or no indication of recovery, resection is indicated. If the organ shows
ultrasonography, but often they can be revealed only through sur- partial recovery within 10 minutes after the pedicle is untwisted, a](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-7-320.jpg)
![© 2006 WebMD, Inc. All rights reserved. ACS Surgery: Principles and Practice
5 GASTROINTESTINAL TRACT AND ABDOMEN 31 Appendectomy — 8
Table 1—Results of 31 Prospective, Randomized
Trials Comparing Laparoscopic Appendectomy with
Open Appendectomy31-61
Laparoscopic Appendectomy Open Appendectomy
Variable (N=2,194) (N=2,158)
No. Range No. Range
Negative appendix 314 (14.3%) 7.7%–36.0% 319 (14.8%) 0%–35.5%
Conversion to open procedure 223 (10.2%) 0%–23.9% NA NA
Surgical site infection 77 (3.5%) 0%–18.3% 144 (6.7%) 0%–17.3%
Intra-abdominal abscess 55 (2.5%) 0%–7.4% 24 (1.1%) 0%–4.6%
Days in hospital 2.7 1–4.9 3.2 1.2–5.3
second-look laparoscopy is indicated in 24 hours. Pelvic inflam- In men and children with suspected acute appendicitis, laparo-
matory disease should be treated on an individualized basis in scopic appendectomy has no major advantage over open appen-
accordance with the degree of inflammation, the patient’s age and dectomy.37 In women of childbearing age and in equivocal cases,
desire to have children, and the microbiologic findings. laparoscopy may be valuable as a diagnostic tool, but the practice
of not removing a normal-looking appendix during exploration for
right lower quadrant pain is controversial. Laparoscopic appen-
Complications and Outcome Evaluation dectomy appears to offer the potential benefit of less postoperative
adhesion formation, but the evidence is inconclusive in the light of
OPEN VERSUS LAPAROSCOPIC APPENDECTOMY
the short follow-up times reported in these trials, and the higher
To date, 31 reports of randomized, controlled trials comparing incidence of intra-abdominal abscess formation remains cause for
laparoscopic appendectomy with open appendectomy have been concern. To date, unfortunately, there have been no studies
published as full manuscripts in English [see Table 1].31-61 These designed specifically to address reduced adhesion formation as a
reports involved a total of 4,352 patients, of whom 2,194 under- primary end point.
went laparoscopic appendectomy and 2,158 underwent open Although laparoscopic appendectomy is being performed with
appendectomy. The incidence of histologically normal appendix increased frequency, it continues to be used selectively. The lap-
was similar in the two groups (14.3% with laparoscopic appendec- aroscopic version of the procedure is at least as safe as the corres-
tomy versus 14.8% with open appendectomy).The conversion rate ponding open procedure, but it is undeniably more time-consum-
from laparoscopic appendectomy to open appendectomy was 10% ing and more costly. Moreover, it remains questionable whether the
(range, 0% to 23%). Laparoscopic appendectomy was associated benefits of laparoscopic appendectomy—reduced postoperative pain,
with a lower incidence of postoperative wound infection than open earlier resumption of oral feeding, shortened hospital stay, quicker
appendectomy was (3.5% versus 6.7%), but it was also associated return to normal preoperative activities, and lower incidence of sur-
with a higher incidence of postoperative intra-abdominal abscess gical site infection—outweigh the doubled incidence of postopera-
(2.5% versus 1.1%). The length of stay was slightly shorter after tive intra-abdominal abscess formation. Further randomized clini-
laparoscopic appendectomy (1 to 4.9 days; average, 2.7 days) than cal studies focusing on the efficacy of laparoscopic appendectomy
after open appendectomy (1.2 to 5.3 days; average, 3.2 days). as a diagnostic tool and on the incidence of postoperative intra-
Randomized, controlled trials carried out within the past 5 years abdominal abscess and adhesion formation are needed, as are addi-
have not led to any significant changes in the statistical picture. tional cost analyses.
References
1. Fitz RH: Perforating inflammation of the vermi- 6. Knight PJ, Vassy LE: Specific diseases mimicking gross appearance at appendix and histological
form appendix with special reference to its early appendicitis in childhood. Arch Surg 116:744, examination. Ann R Coll Surg Edinb 70:395, 1988
diagnosis and treatment. Trans Assoc Am 1981
12. Blair PM, Bugis PS, Turner LJ, et al: Review of the
Physicians 1:107, 1886 7. Pieper R, Kager L, Nasman P: Acute appendicitis: pathologic diagnosis of 2,216 appendectomy speci-
2. McBurney C: The incision made in the abdominal a clinical study of 1,018 cases of emergency appen- mens. Am J Surg 165:618, 1993
wall in cases of appendicitis, with a description of a dectomy. Acta Chir Scand 148:51, 1982
new method of operating. Ann Surg 20:38, 1894 13. Dahlstom JE, MacArthur EB: Enterobius vermicu-
8. Arnbjornsson E, Asp NG, Westin SI: Decreasing laris: a possible cause of symptoms resembling
3. Rucinski J, Fabian T, Panagopoulos G, et al: incidence of acute appendicitis, with special refer-
appendicitis. Aust NZ J Surg 64:692, 1994
Gangrenous and perforated appendicitis: a meta- ence to the consumption of dietary fiber. Acta Chir
analytic study of 2532 patients indicates that the Scand 148:461, 1982 14. Pearl RH, Hale DA, Molloy M, et al: Pediatric
incision should be closed primarily. Surgery 9. Blind PJ, Dahlgren ST:The continuing challenge of appendectomy. J Pediatr Surg 30:173, 1995
127:136, 2000 the negative appendix. Acta Chir Scand 152:623, 15. Truji M, Puri P, Reen DJ: Characterization of the
4. Flum DR, Morris A, Koepsell T, et al: Has misdiag- 1986 local inflammatory response in appendicitis. J
nosis of appendicitis decreased over time? a popula- 10. Lau WY: Correlation between gross appeareance of Pediatr Gastroenterol Nutr 16:43, 1993
tion-based analysis. JAMA 286:1748, 2001 the appendix and histological examination. Ann R 16. Wang Y, Reen DJ, Puri P: Is a histologically normal
5. Chang AR: An analysis of the pathology of 3,003 Coll Surg Edinb 70:336, 1988 appendix following emergency appendicectomy
appendices. Aust NZ J Surg 51:169, 1981 11. Budd JS, Armstrong CP: The correlation between always normal? Lancet 347:1076, 1996](https://image.slidesharecdn.com/acs0531-appendectomy-2006-100726063427-phpapp01/85/Acs0531-Appendectomy-2006-8-320.jpg)

















































![APPENDICITIS Nursing managment[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/appendicitisautosaved-250207063037-951fd6a3-thumbnail.jpg?width=640&height=640&fit=bounds)