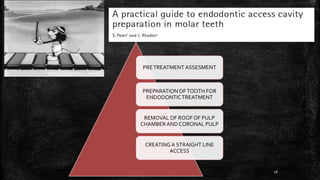
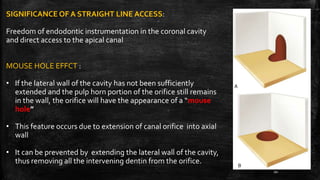
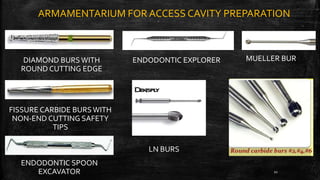
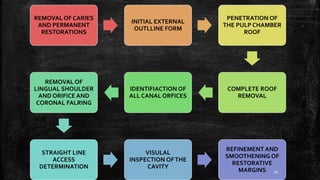
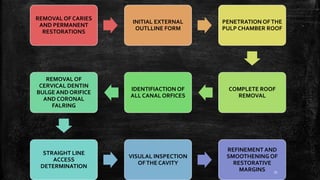
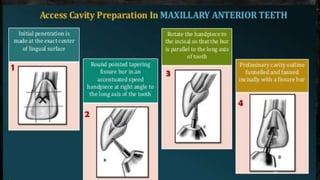
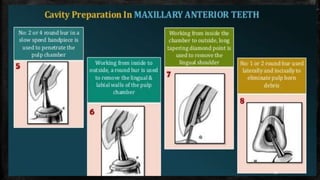
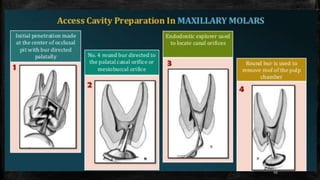
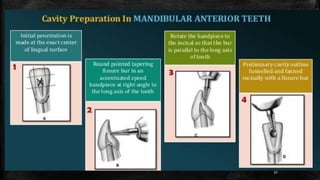
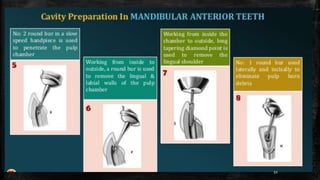
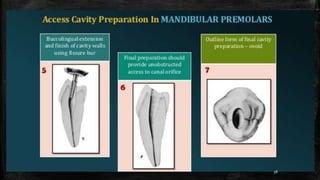
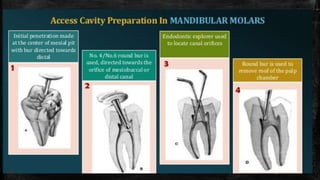
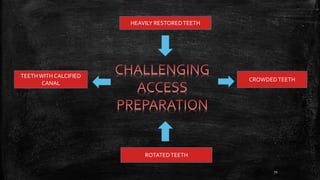
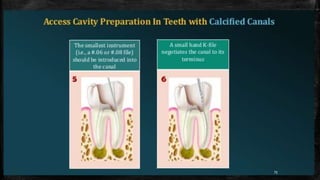
1. Access cavity preparation is the first and most important step in root canal treatment as it provides straight-line access to the root canals.
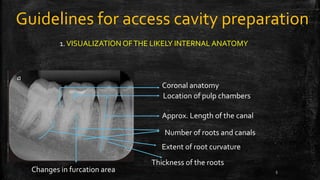
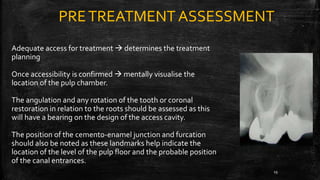
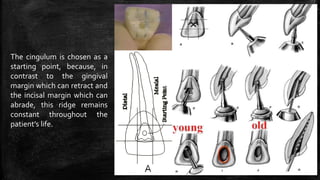
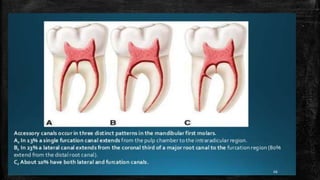
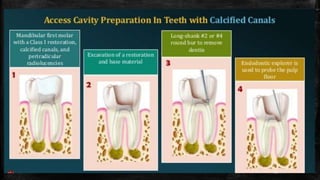
2. Anatomical landmarks like the cementoenamel junction and root development lines can help locate canal orifices.
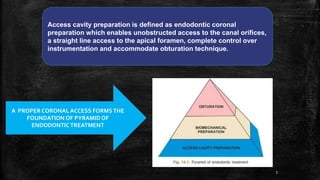
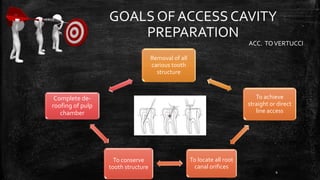
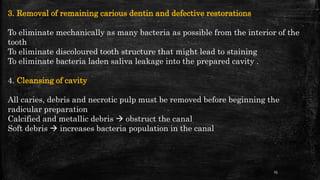
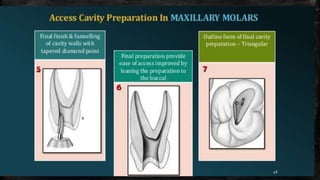
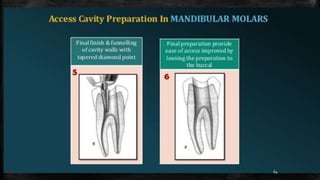
3. The goals of access cavity preparation are to remove all caries, locate all root canals, and achieve a conservative cavity that provides direct access to the canals and apical foramen.
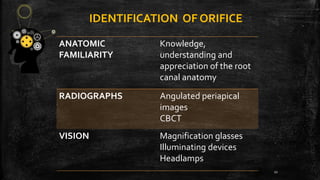
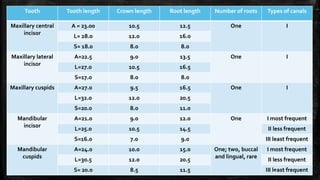
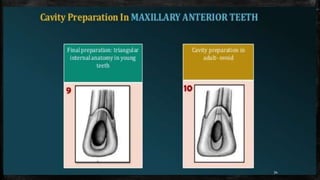
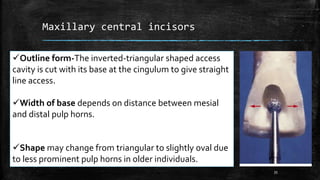
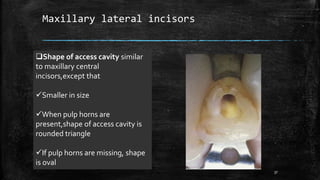
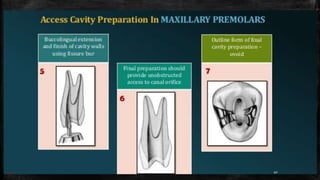
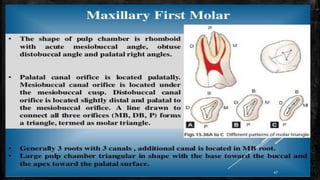
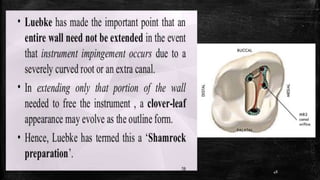
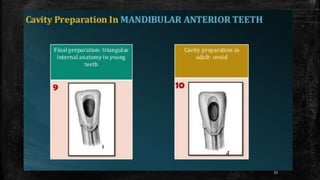
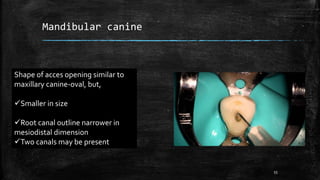
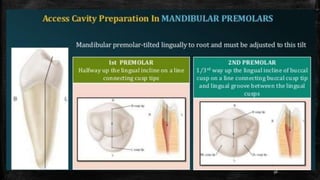
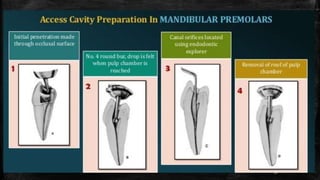
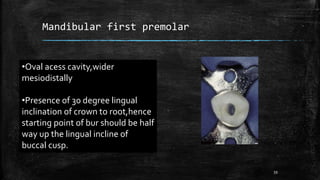
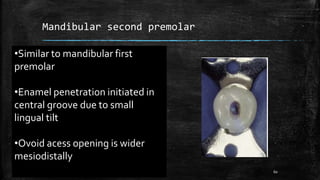
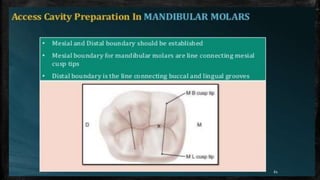
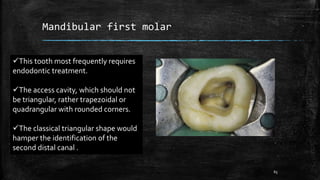
4. The shape and size of the access cavity varies between teeth based on their anatomy and number of canals. Proper identification of canal orifices is crucial for successful root canal treatment.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













