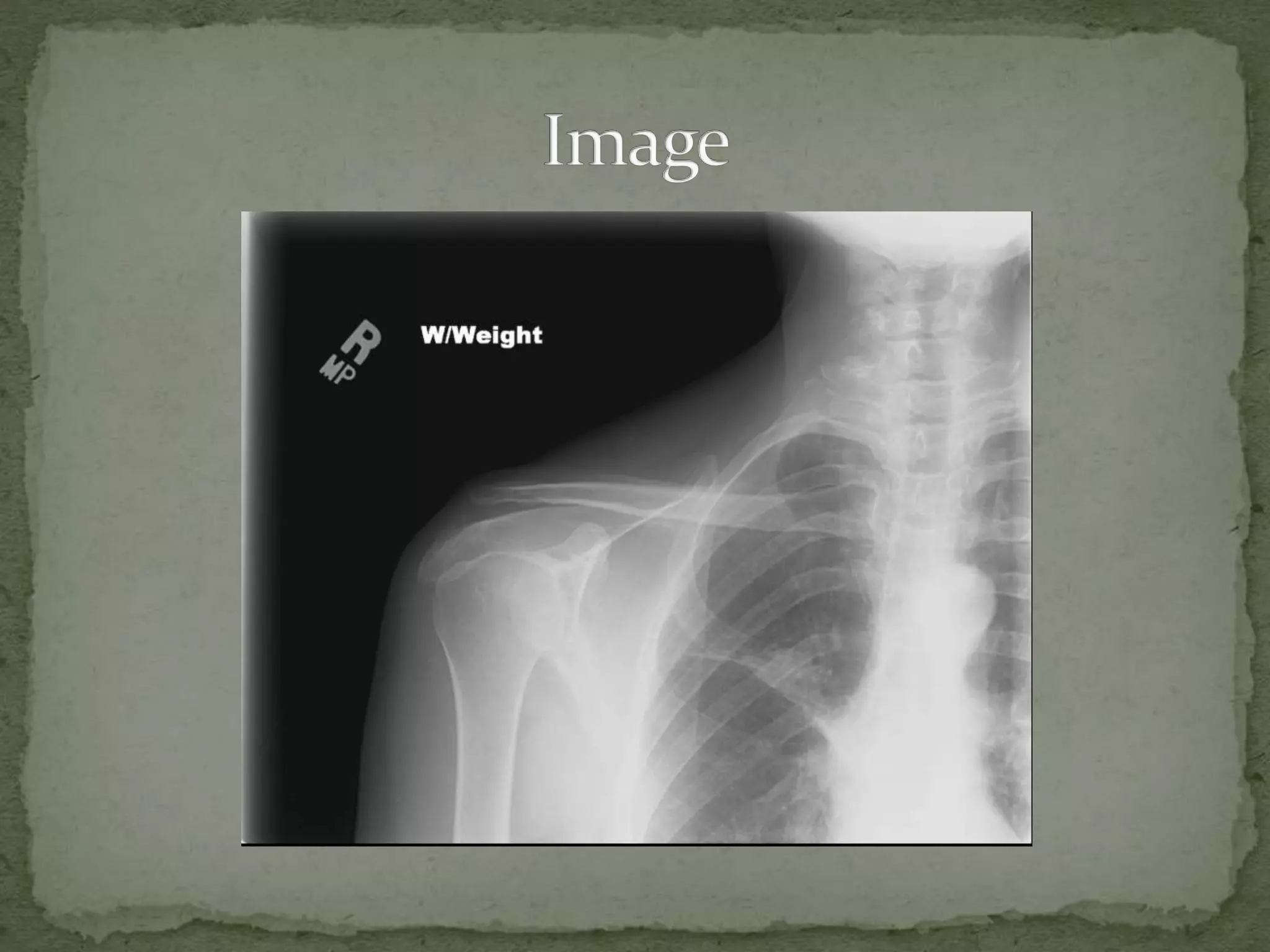
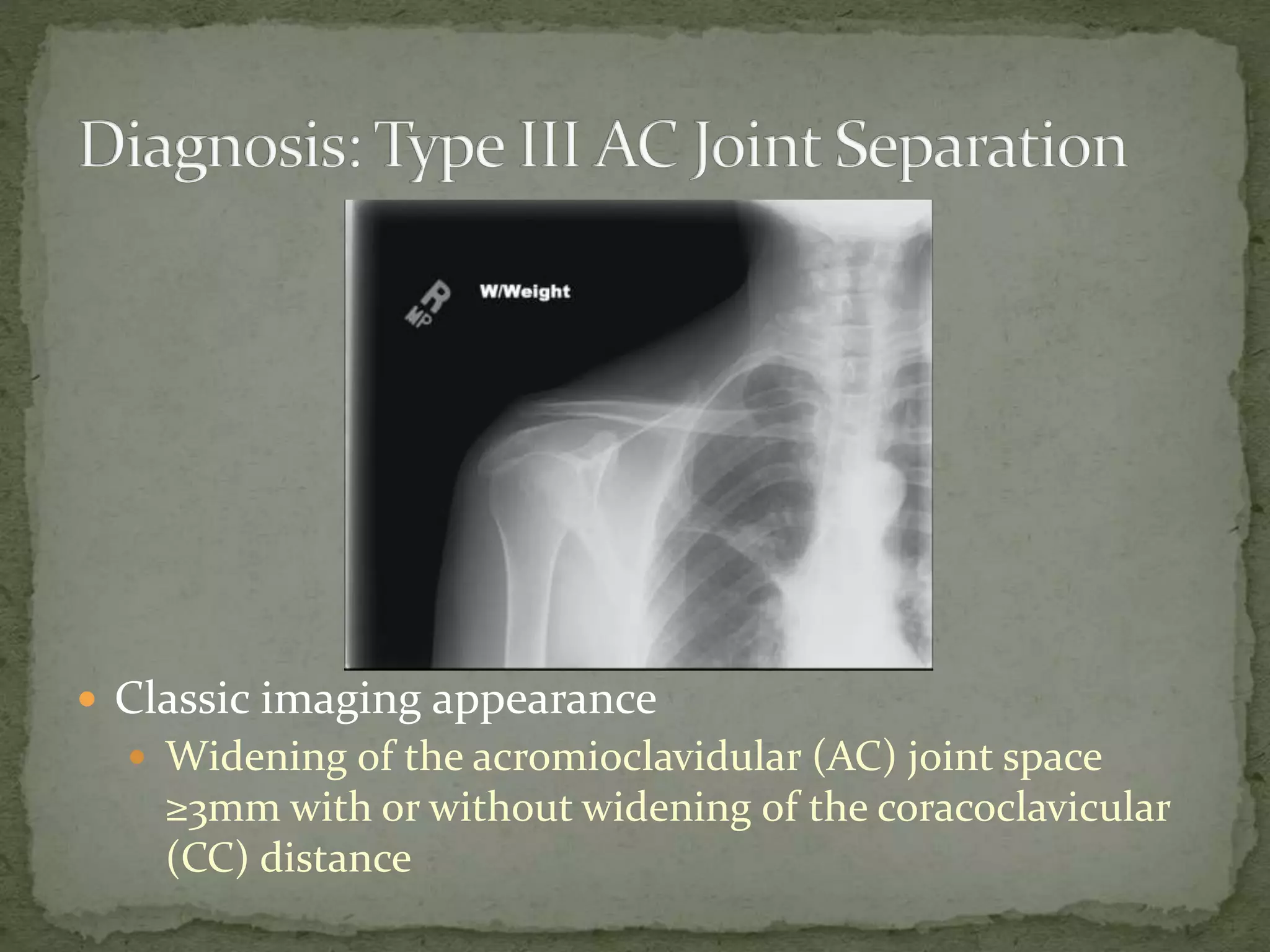
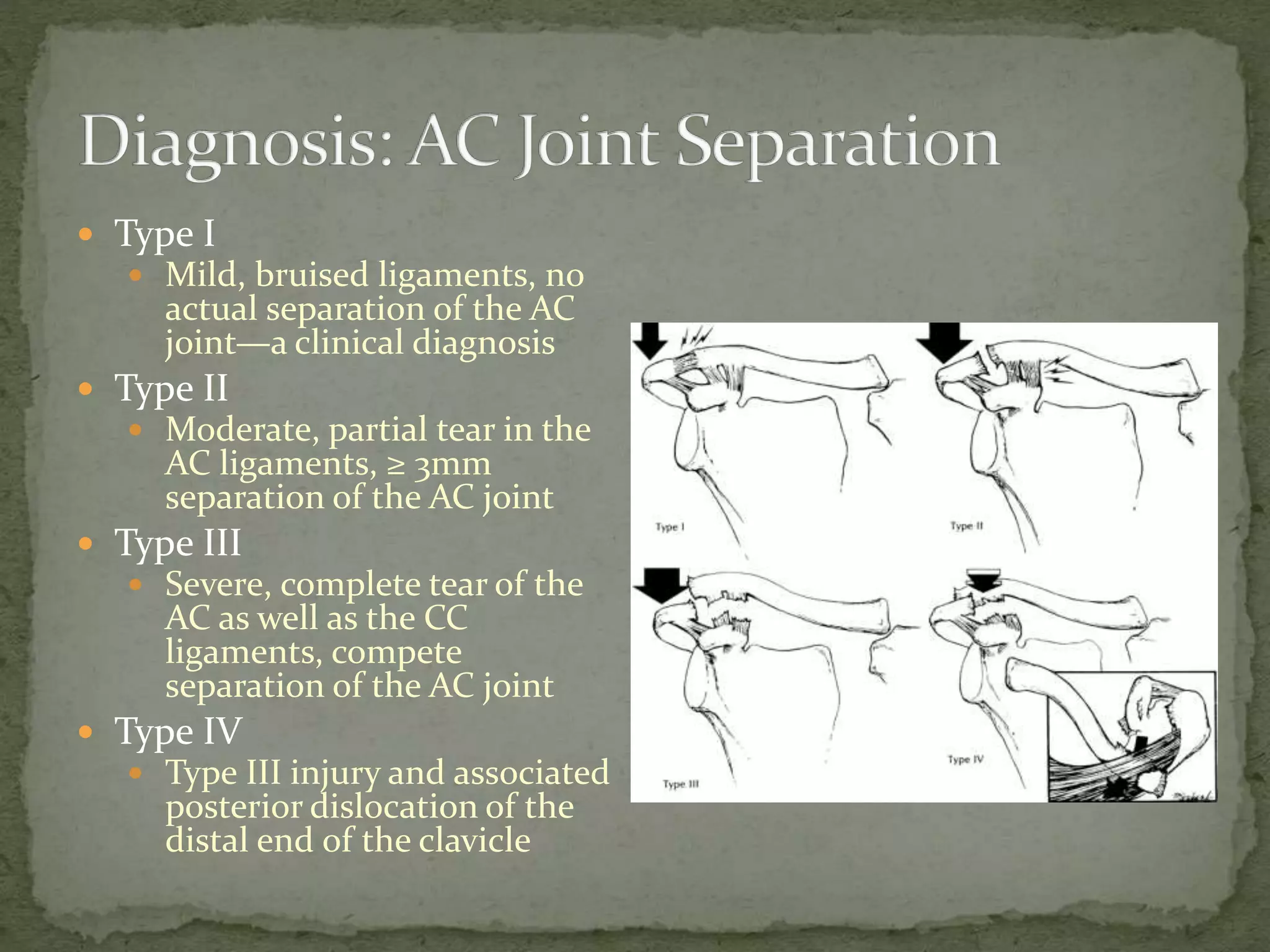
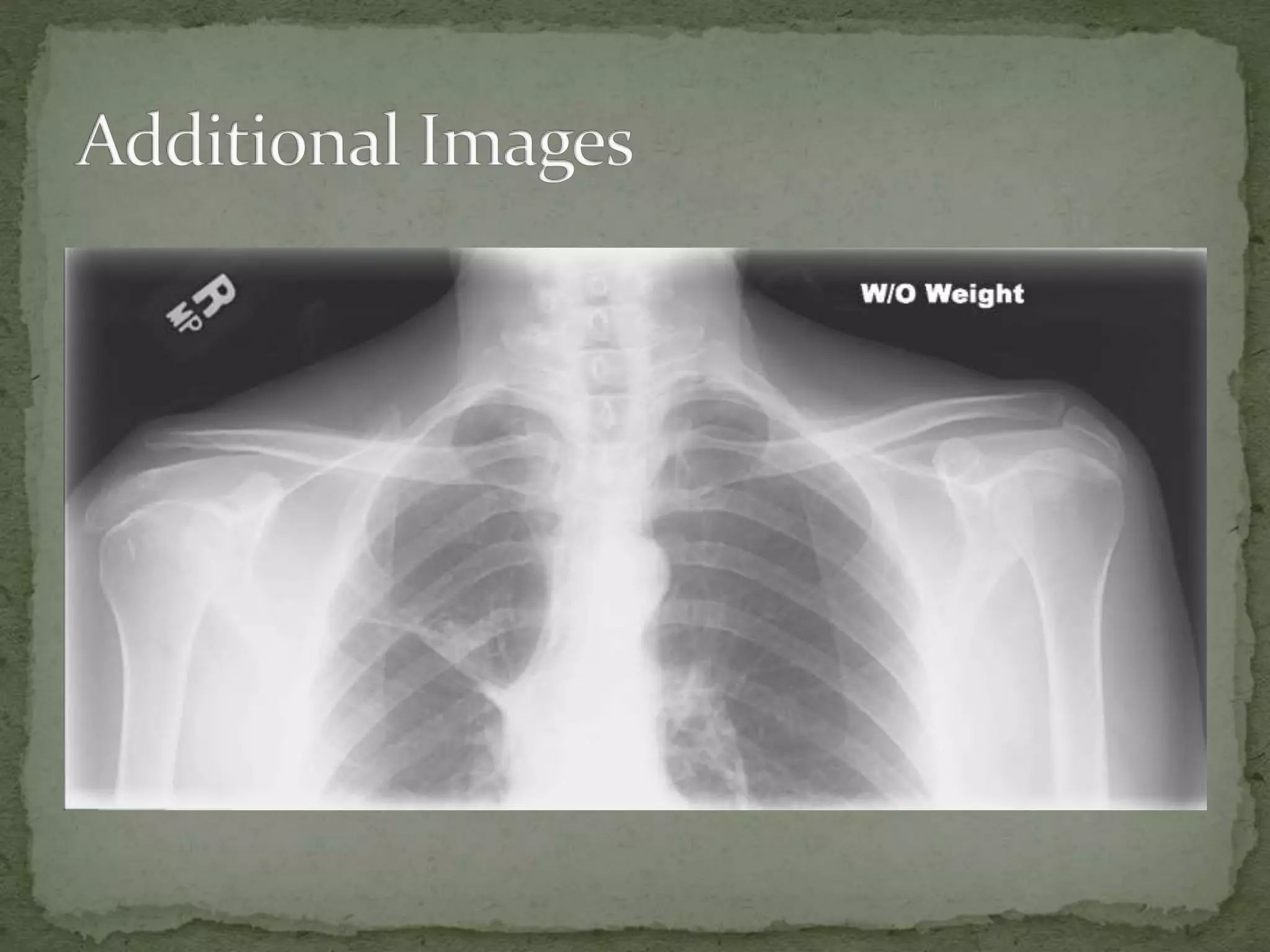
A 42-year-old man presented to the emergency department after being struck in the right shoulder with a baseball bat. On exam, he refused to move his shoulder due to pain and tenderness over the top of the shoulder. Imaging showed widening of the acromioclavicular joint space, indicating an AC joint separation. The separation was likely a Type III injury, with a complete tear of the AC and coracoclavicular ligaments and separation of the AC joint, requiring internal fixation surgery to repair the injury.