Downloaded 59 times






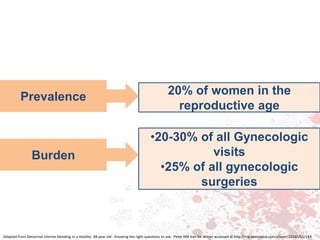







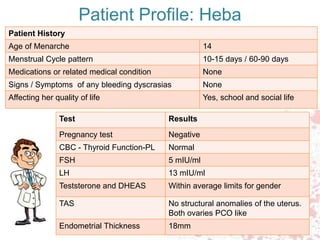






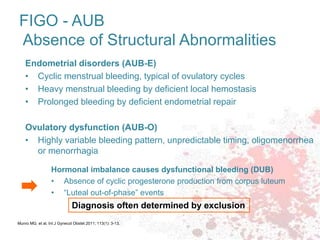























The document discusses abnormal uterine bleeding (AUB) in two patients: Mrs. Aisha, a 48-year-old teacher with heavy menstrual bleeding, and Miss Heba, a 16-year-old school girl presenting with similar symptoms. It examines various causes, diagnostic approaches, and treatment options for AUB, highlighting the importance of understanding individual factors when determining management strategies. Progestagens are emphasized as an effective treatment for anovulatory causes of heavy menstrual bleeding, with the need for ongoing assessment and tailored care.