INTRODUCTION
• Any uterinebleeding outside the normal volume, duration, regularity or
frequency is considered abnormal uterine bleeding (AUB).
• AUB accounts for nearly 30% of all gynecological outpatient attendants.
• Recall that a normal menstrual cycle occurs every 21-35 days (28 +/- 7 days)
with menstruation for 2-7 days.
• The normal blood loss is less than 80ml total (20-80 ml with an average of
35ml) which represents 8 or fewer soaked pads per day with usually no more
than 2 heavy days.
4.
INTRODUCTION cntd
• AUBpattern have been traditionally expressed by terms like
menorrhagia, metrorrhagia, polymenorrhea and oligomenorrhea
however, in order to create a universally accepted nomenclature to
describe AUB the International Federation of gynecology and obstetrics
(FIGO) and American College of Obstetricians and Gynecologists
(ACOG) introduced newer system of terminology to describe AUB.
5.
Classification of causes
•This new classification system is known by the acronym PALM-COEIN
➢ P- poly (AUB-P)
➢ A-adenomyosis (AUB-A)
➢ L- leiomyoma (AUB-L)
➢ M- malignancy and hyperplasia (AUB-M)
➢ C- coagulopathy (AUB-C)
➢ O- ovulatory dysfunction (AUB-O): oligovulation, anovulation,
polycystic changes and corpus luteum dysfunction.
6.
Classification cntd
➢ E-endometrial (AUB-E): chronic endometritis, infection and endometrial vascular
pathology (angioma). Primary disorders of the endometrium may cause AUB or DUB.
Imbalance in levels of different hemostatic mechanisms may be responsible for AUB.
Optimum levels of endothelin I, PG F2 alpha, formation of platelet plug or fibrin seal are
essential to control bleeding. Excess production of plasminogen activators, production
of substances that promote vasodilation (PG E2, I2) may result in AUB.
➢ I-iatrogenic (AUB-I): breakthrough bleeding following use of Oral contraceptives,
erratic use of pills or any contraceptive steroids (vaginal rings), use of IUCDs or LNG-IUS.
➢ N-not yet classified (AUB-N)
• Dysfunctional uterine bleeding (DUB) is a type of AUB, whereas no system or locally
identifiable structural cause is found.
7.
MENORRHAGIA- Heavy menstrualbleeding (HMB)
• Menorrhagia is defined as cyclical regular uterine blood loss greater
than 80ml per period or duration >7 days or both.
• Heavy menstrual bleeding (HMB) is now the preferred description as it
is simple and easily translatable into other languages.
• The term menotaxis is often used to denote prolonged bleeding.
• It can occur at any age however is common in women between the
age of 30 to 49.
8.
ETIOLOGY
ETIOLOGY
• Can beclassified as:
➢ Organic causes
➢ Functional causes
ORGANIC CUASES
PELVIC
• Fibroid uterus (common)
• Pelvic endometriosis (common)
• Adenomyosis (common)
• PID and Chronic tubo-ovarian mass (common)
• Endometrial and cervical carcinoma
• IUCD inutero
• TB endometritis (Early cases)
• Endometrial polyps
• Retroverted uterus (due to congestion)
• Granulosa cell tumor of the ovary (excess
estrogen)
• Endometrial and cervical carcinoma
• IUCD inutero
• TB endometritis (Early cases)
• Endometrial polyps
• Retroverted uterus (due to congestion)
• Granulosa cell tumor of the ovary (excess
estrogen)
9.
SYSTEMIC CAUSES
SYSTEMIC
• Liverdysfunction- failure to conjugate and thereby inactivates the
estrogens
• Severe hypertension
• Congestive cardiac failure
FUNCTIONAL
• Due todisturbed hypothalamo-pituitary-ovarian-endometrial axis
• To help remember the causes of abnormal uterine bleeding recall the mnemonic
“PALM-COEIN”
➢ P-polyp
➢ A-Adenomyosis
➢ L-Leiomyoma (uterine fibroid)
➢ M- Malignancy and hyperplasia
➢ C-Coagulopathy (vonWille brand disease)
➢ O-ovulatory dysfunction
➢ E-Endometrial
➢ I-iatrogenic
➢ N-not yet classified
12.
CLINICAL FEATURES
• Longduration of flow
• Passage of big clots
• Use of increased number of thick sanitary pads (usually more than 8
pads used with more than 2 soaked heavily per day), pallor
• Signs and symptoms of anemia
14.
HISTORY AND EXAMINATION
HISTORY
•Ask details about the menstrual cycle
➢ Last menstrual period
➢ What is the duration? (typical 21 to 35 days)
o <21 days= polymenorrhea
o >35 days= oligomenorrhea
➢ Is it regular?
• How long has the bleeding been for?
• When was it first noticed?
• How often does soaked sanitary wear need to be changed?
• Is there any of clots?
15.
History..
• Is thebleeding so heavy (flooding) that it spills over your towel/tampon and on
to your pants, clothes or bedding?
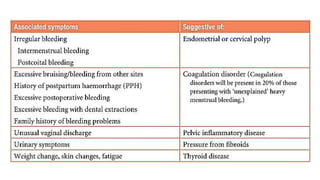
• Any intermenstrual bleeding or post-coital bleeding? (cervical lesion or polyp,
glandular tissue on cervix)
• Any pain associated with the bleeding? (endometriosis, adenomyosis)
• Have you had to take any time off work due to this bleeding?
• Do you ever find you are confined to your house when the bleeding is at its
worst?
• Any unusual vaginal discharge?
• Contraceptive history- copper IUCD (increase bleeding)
• Do you have any of the following symptoms:
➢ Dizziness, Lightheadedness, Headache, Heart palpitations, Fainting
16.
History..
• Personal andfamily history of fibroids?
• Family history of bleeding?
• Epistaxis, gum bleeding, postpartum bleeding, surgical bleeding?
• Cold intolerance or heat intolerance?
17.
EXAMINATION
• After examiningthe patient for sings of anemia, it is important to perform
an
abdominal and pelvic examination in all women with menorrhagia.
• This enables any pelvic masses to be palpated, the cervix to be visualized for
polyps/carcinoma, swabs to be taken if pelvic infection is suspected or a
cervical smear to be taken if one is due.
• Bimanual may reveal bulky uterus/discrete fibroids.
• Exophthalmos, goiter, delayed DTRs, dry skin/hair (thyroid disorder)
• Petechiae (coagulopathy)
18.
INVESTIGATIONS
• Pregnancy test
•Full blood count- anemia and need for transfusion
• Clotting profile- to rule out clotting disorders
• Hormones: Testosterone, TSH, T3, T4, FSH, LH and prolactin
• Pelvic ultrasound:
➢ Fibroids (pelvic mass palpated on exam)
➢ When symptoms suggest an endometrial polyp e.g. irregular or
intermenstrual bleeding
➢ When drug therapy for menorrhagia is unsuccessful
19.
INVESTIGATIONS...
• High vaginaland Endocervical swabs
➢ When unusual vaginal discharge is reported or observed in examination
➢ When there are risk factors for PID
• Endometrial biopsy (outpatient hysteroscopy with endometrial biopsy)
➢ All patients >45 years
➢ If irregular, intermenstrual bleeding, or persistent abnormal uterine
bleeding (patient <45 years)
➢ Drug therapy has failed.
• PAP smear
• Hysteroscopy
20.
MANAGEMENT
• Dependent oncause.
• Effectiveness of medical treatment is often temporary while surgical treatments
are mostly incompatible with desired fertility.
• During treatment consider
➢ Patient’s preference of treatment
➢ Risks/benefits of each option
➢ Contraceptive requirements
o Family complete?
o Current contraception?
➢ Past medical history:
o Any contraindications to medical therapies for heavy menstrual bleeding
o Suitability for an anaesthetic, previous surgical history?
21.
MEDICAL THERAPY
• Mefenamicacids and other non-steroidal anti-inflammatory drugs (NSAIDs)
associated with reduction in mean menstrual blood loss of 20-25%.
➢ Dose: 500mg PO once then 250mg PO every 6 hours as required/ PRN (do not
exceed 3 days).
➢ Mechanism of action: this is a non-steroidal anti-inflammatory drug it helps
reduce pain (Analgesic), inflammation and bleeding by inhibiting the
production of prostaglandins via the cyclo-oxygenase pathway
➢ Benefits: effective analgesia, hence often the first line treatment of choice
where dysmenorrhea co-exists
➢ Disadvantages: contraindicated with a history of duodenal ulcer or severe
asthma
22.
MEDICAL THERAPY...
• Tranexamicacid: associated with mean reduction in menstrual blood loss of
about 50%
➢ Dose: 1g PO TDS for up to 4 days to be initiated when menstruation has
started (maximum 4g per day)
➢ Mechanism of action: inhibits plasminogen activation thus plasminogen is
not activated to plasmin and it cannot catalyze the conversion of fibrin to its
degradation products this promotes hemostasis.
➢ Benefits: only requires to be taken on days when bleeding is particularly
heavy. Compatible with ongoing attempts at conception.
23.
MEDICAL THERAPY...
• Combinedoral contraceptive pill 340
➢ Mechanism of action: low level estrogen in the pills provides a constant negative feedback on the
pituitary and hypothalamus thus reducing the production of gonadotrophins which results an
amenorrhoic state
➢ Benefits: doubles up as very effective contraceptive when taken properly
➢ Disadvantage: contraindication in patients with risk for thromboembolism, hypertension, not
suitable for patients over 35years who smoke, if there is a personal or family history of breast
cancer and in patients who are grossly overweight
• Norethisterone: cyclical progestogen is effective taken in a cyclical pattern from day 6 to day 26 of
the menstrual cycle.
➢ Dose 5-10mg TDS on days 6-26 of the menstrual cycle.
➢ Benefits: safe and effective oral preparation which can regulate bleeding pattern
➢ Disadvantage: it is not a contraceptive and can cause break-through bleeding.
• Other medical treatment: Levonogesterel intrauterine system, and Gonadotropin releasing
hormone agonists.
24.
SURGICAL THERAPY
• Indications:
➢Failed medical treatment
➢ Satisfied parity
• Dilatation and curettage: Indicated mainly for women with heavy bleeding
leading to hemodynamic instability.
• Endometrial ablation: used as an alternative to hysterectomy when medical
modalities fail or when there are contraindications to their use. It should not be
used in women who wish to maintain their reproductive capacity. ablation of the
endometrial lining of the uterus to sufficient depth prevents regeneration of the
endometrium and reduces blood loss by 90%.
• Myomectomy
• Hysterectomy: reserved for woman with other indications for hysterectomy,
such as leiomyomas or uterine prolapse.
25.
COMPLICATIONS
• Microcytic hypochromicanemia
• High output cardiac failure
• Recurrent genital tract infection
• Psychological social withdrawal and inability to progress in school or
be effective at work
26.
METRORRHAGIA
• This isirregular acyclic bleeding between periods from the uterus.
• The amount is variable
• Contact bleeding or intermenstrual bleeding in an otherwise normal
cycle is also included in metrorrhagia.
• Menometrorrhagia is the term applied when the bleeding is so irregular
and excessive that the menses (periods) cannot be identified at all.
27.
Causes of metrorrhagia:
➢Acyclic bleeding:
o Dysfunctional uterine bleeding- usually during
adolescence, following childbirth and abortion
and preceding menopause.
o Submucous fibroid
o Uterine polyp
o Carcinoma cervix and endometrial carcinoma
➢ Contact bleeding
o Carcinoma cervix
o Mucous polyp of cervix
o Vascular ectopy of the cervix especially during
pregnancy, pill use cervix
o Infections-chlamydial or tubercular cervicitis
o Cervical endometriosis
➢ Intermenstrual bleeding
o IUCD in utero
o Breatkthrough bleeding in pill use
o Urethral caruncle
o Ovular bleeding
• Treatment: directed to the underlying pathology.
Malignancy is to be excluded
prior to any definitive treatment.
28.
POLYMENORRHEA (EPIMENORRHEA)
• Thisis cyclic bleeding where the cycle is reduced to an arbitrary limit of less
than 21 days and remains constant at that frequency.
• If the frequent cycle is associated with excessive and/or prolonged bleeding it
is called epimenorrhagia.
Causes:
➢ Dysfunctional: seen during adolescence, preceding menopause and
following delivery and abortion. Hyperstimulation of the ovary by pituitary
hormones may be the responsible factor.
➢ Ovarian hyperemia: PID or Ovarian endometriosis
• Treatment: persistent dysfunctional type is treated by hormones as outlined in
dysfunctional uterine bleeding.
29.
OLIGOMENORRHEA
• This ismenstrual bleeding occurring more than 35 days apart and which
remain constant at that frequency.
Causes:
➢ Age-related: during adolescence and preceding menopause
➢ Weight related-obesity
➢ Stress and exercise related
➢ Endocrine disorders- PCOS (commonest), hyperprolactinemia,
hyperthyroidism
➢ Androgen producing tumors-ovarian, adrenal
➢ Tubercular endometritis
➢ Drugs: phenothiazines, cimetidine, methyldopa
30.
HYPOMENORRHEA
• This occurswhen the menstrual bleeding is unduly scanty and lasts for less than 2
days.
Causes:
➢ Local:
o Uterine synechiae
o Endometrial tuberculosis
➢ Endocrinal:
o Use of oral contraceptives
o Thyroid dysfunction
o Premenopausal period
➢ Systemic: malnutrition
31.
DYSFUNCTIONAL UTERINE BLEEDING
•This is a state of abnormal uterine bleeding without any clinically detectable
organic, systemic and iatrogenic cause (pelvic pathology e.g. tumor,
inflammation or pregnancy is excluded).
• It accounts for 10% of new patients attending the OPD.
• Currently DUB is defined as a state of abnormal uterine bleeding following
anovulation due to dysfunction of hypothalamo-pituitary-ovarian axis
(endocrine origin)
• DUB can be:
➢ Ovulatory: associated with ovulation(10%)
➢ Anovulatory: not associated with ovulation(80%)
32.
PATHOPHYSIOLOGY
• Recall: thephysiological mechanism of hemostasis in normal menstruation are:
➢ Platelet adhesion formation
➢ Formation of platelet plug with fibrin to seal the bleeding vessels
➢ Localized vasoconstriction
➢ Regeneration of endometrium
• Biochemical mechanisms involved:
➢ Increased endometrial ratio of PGF 2 alpha/ PGE2.
➢ PGF 2 alpha causes vasoconstriction and reduces bleeding
➢ Progesterone increases the level of PGE 2 alpha from arachidonic acid.
➢ Levels of endothelin which is a powerful constrictor is also increased
• In anovulatory DUB there is decreased synthesis of PGF 2 alpha and the ratio of PGF 2alpha/PGE 2 is low.
Anovulatory cycles are usually not associated with dysmenorrhea as the level of PGF2 alpha is low.
➢ Recall prostaglandins stimulate the contraction of the uterus and thereby giving rise to the cramping, if not
present then bleeding is not associated with pain.
33.
PATHOPHYSIOLOGY....
• Women withmenorrhagia have low level of thromboxane in the
endometrium.
• The endometrial abnormalities may be primary or secondary to
incoordination in the hypothalamo-pituitary-ovarian axis. It is therefore
more prevalent in the extremes of reproductive period- adolescence
and premenopause or following childbirth and abortion.
• Emotional influences, worries, anxieties or sexual problems
sometimes are enough to disturb the normal hormonal balance.
34.
OVULATORY BLEEDING
• Polymenorrheaor polymenorrhagia: usually follows child birth and abortion,
during adolescence and premenopausal period and in pelvic inflammatory
disease. The follicular development is speeded up with resulting shortening of
the follicular phase. This probably due to hyperstimulation of the follicular
growth by FSH. Rarely, the luteal phase may be shortened due to premature
lysis of the corpus luteum. Sometimes it is related to stress induced
stimulation.
• Oligomenorrhea: primary ovular oligomenorrhea is rare. It may be met in
adolescence and preceding menopause. The disturbance may be due to ovarian
unresponsiveness to FSH or secondary to pituitary dysfunction.
35.
ANOVULATORY BLEEDING
• Menorrhagia:anovular bleeding is usually excessive. In the absence of growth
limiting progesterone due to anovulation, the endometrial growth is under the
influence of estrogen throughout the cycle. There is inadequate structural
stromal support and the endometrium remains fragile (unstable). Withdrawal
of estrogen due to negative feedback action of FSH, the endometrial shedding
continues for a longer period in asynchronous sequences because of lack of
compactness.
36.
Cystic glandular hyperplasia(Metropathia
hemorrhagica, Schroeder’s disease
• This is abnormal bleeding usually seen in premenopausal women.
• The pathology may be in the ovaries or due to disturbance of the rhythmic
secretion of gonadotrophins. There is slow increase in secretion of estrogen but
no negative feedback inhibition of FSH. The net effect is gradual rise in the level
of estrogen with concomitant phase of amenorrhea for about 6-8 weeks.
• As there is no ovulation, the endometrium is under the influence of estrogen
without being opposed by growth limiting progesterone for a prolonged period.
After a variable period, however, the estrogen level falls resulting in endometrial
shedding with heavy bleeding. Bleeding also occurs when the endometrial
growth have outgrown their blood supply. Due to increased endometrial
thickness, tissue breakdown continues for a long time. Bleeding is heavy as there
is no vasoconstrictor effect of PGF 2 alpha.
• Bleeding is prolonged until the endometrium and blood vessels regenerate to
control it.
37.
Cystic glandular hyperplasia...
➢ Uterine changes: variable degree of myohyperplasia with
symmetrical enlargement of the uterus to a size of about 8-10 weeks
due to simultaneous hypertrophy of muscles. The endometrium looks
congested and polypoidal (multiple polyposis).
38.
Cystic glandular hyperplasia...
➢ Microscopic uterine changes:
o Hyperplasia of all endometrial components.
o Intense cystic glandular hypertrophy rather than hyperplasia with
marked disparity in sizes. Some glands are small, other are large giving
the appearance of “Swiss cheese” pattern (small and large holes of
Swiss cheese made in Switzerland). The glands are empty and lined by
columnar epithelium
o Absence of secretory changes
o Areas of necrosis in superficial layers with small hemorrhages and
leukocytic infiltration
39.
Cystic glandular hyperplasia...
➢ Ovary changes: cystic changes in one or both ovaries. Cysts may be
single or multiple and fluid contains estrogen. The cyst is of follicular
type. There is no evidence of corpus luteum
40.
Cystic glandular hyperplasia...
• Atrophy of endometrium: seen in postmenopausal women and during the
reproductive period as final involutionary state of a previous metropathia.
Bleeding occurs from rupture of the dilated capillaries beneath the atrophic
surface epithelium. Endometrial atrophy may be caused by total absence of
estrogen or failure of uterine receptors to become responsive to estrogen.
Note: DUB of anovulatory type is painless due to decreased synthesis of PGF
2 alpha (PGF 2 alpha/PG E2 is low) and thromboxane. This can differentiate
the amenorrhea followed by bleeding per vagina with a bulky uterus seen with
a disturbed pregnancy or ectopic pregnancy.
41.
HISTORY AND EXAMINATION
•Age,number of pads,clots,duration of
bleeding,acyclic,cyclic,continuous,pain,contraceptives,abnormal
bleeding
• General and relevant systemic examination to find out cause or
effect of abnormal bleeding
• Bimanual examination including speculum examination should be
done in all cases except in virgins where rectal examination is done
to exclude palpable pelvic pathology.
42.
INVESTIGATIONS
• Blood:
➢ Fullblood count
➢ Coagulation profile: PT, bleeding time, PTT
➢ Thyroid function test for thyroid pathology
• Imaging
➢ Ultrasound and color doppler: endometrial hyperplasia (endometrial thickness >12mm, hyperechoic and
regular, angiogenesis and neovascular signal study). Transvaginal is sensitive at detecting anatomical
abnormalities (fibroid, adenomyosis) of the uterus, endometrium and adnexae.
➢ Saline infusion sonography: useful in endometrial polyps, submucous fibroids and uterine abnormality
(septate/subseptate uterus)
➢ Hysteroscopy- good for endometrial lesions and biopsy can be taken, this has replaced Dilatation and
curettage.
➢ Endometrial sampling: can be done as an outpatient procedure. Pipelle sampler is easy to used. As it is a
blind procedure, intrauterine pathology (polyps, submucous fibroids) cannot be detected.
➢ Laparoscopy: to exclude unsuspected pelvic pathology such as endometriosis, PID or ovarian tumor
(granulosa cell tumor). The indication is urgent, if associated with pelvic pain
43.
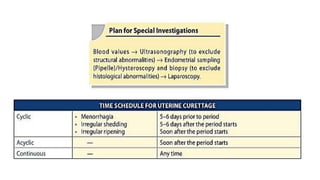
INVESTIGATIONS ...
• Diagnosticuterine curettage (D and C): indicated in DUB to exclude the organic lesions in
the endometrium (incomplete abortion, endometrial polyp, tubercular endometritis or
endometrial carcinoma), to determine the functional state of the endometrium and to have
incidental therapeutic benefit.
➢ In adolescent DUB is rarely needed only if bleeding fails to stop or is severe in nature.
➢ During childbearing period (20-40 years) it should be done if bleeding is acyclic. Risk of
endometrial carcinoma in this age group is low
➢ During premenopausal period, diagnostic curettage is mandatory prior to any therapy to
exclude endometrial malignancy
➢ During post-menopausal period: it is mandatory to exclude endometrial malignancy. Thin
plastic endometrial tissue samplers (pipellae) are available. It helps to obtain adequate
endometrial sample for histological examination. It is done as an OPD procedure without any
anesthetic.
45.
MANAGEMENT
• Depends onthe age
➢ Pubertal and adolescent menorrhagia <20 years
➢ Reproductive period (20-40 years)
➢ Premenopausal (>40 years)
➢ Postmenopausal (discussed later)
46.
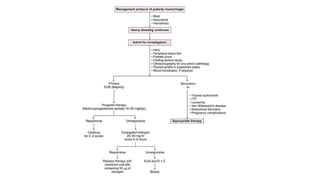
PUBERTAL AND ADOLESCENT
•Adequate explanation, reassurance and psychological support
• Rest and correction of anemia: Hematinics or blood transfusion
• In refractory cases progestogens such as medroxyprogesterone acetate or
norethisterone 5 mg TDS is given till bleeding stops. Usually bleeding is
controlled within 3-7 days. Medication is continued for 21 days. The condition
usually becomes normal following 2-3 courses and then normal cycles resume.
• In emergency, conjugated equine estrogen 20-40 mg IV is given every 6-8
hourly. Once bleeding is controlled, combined oral pills are started.
• Regular menstrual cycle will be established once the hypothalamo-pituitary
ovarian axis is matured.
48.
REPRODUCTIVE PERIOD
• General:
➢Bed rest during bleeding phase
➢ Assurance and sympathy
➢ Correction of anemia: diet, hematinics and blood transfusion
• Medical
➢ Hormones: oral progestins are the mainstay in the management of DUB in all age groups.
o Drugs used: Norethisteron acetate, medroxyprogesterone acetate, dydrogesterone, equine
conjugated estrogen, combined estrogens and progestogens (contraceptive pills), 19 Norsteroid
derivative
(Gestrinone), Danzol (17 alpha ethinyl testosterone), Progestin releasing IUCD LNG-IUS, Mifepristone,
GnRH analogues, desmopressin
o Preparations are used for cyclic therapy or continuous therapy
o To stop bleeding and regulate the cycle use Noretihisterone preparations (5mg tab) TDS till bleeding
stop, which is usually 3-7 days.
49.
Cyclic therapy:
1. 5th,-25th day course:
- In ovular bleeding any low dose combined oral pills are effect when given from 5th to
25th day of cycle for 3 consecutive cycles. It causes endometrial atrophy. It is more
effective compared to progesterone therapy as it suppresses the hypothalamo pituitary
axis more effectively.
- In anovular bleeding: cyclic progestogen preparation of medroxyprogesterone acetate
(MPA) 10mg or norethisterone 5mg is used from 5th to 25th day of the cycle for 3
cycles
2. 15th to 25th day course:
- In ovular bleeding where patient wants pregnancy or in cases of irregular shedding or
irregular ripening of the endometrium, dydrogestrone 1 tab (10 mg) daily or BD from
15th to 25th day may cure the state. This regimen is less effective than 5th to 25th day
course however it does not suppress ovulation
50.
o Continuous therapy:progestins also inhibit pituitary gonadotropin
secretion and ovarian hormone production. Medroxyprogesterone
acetate 10mg TDS is given and treatment is usually continued for at
least 90 days.
➢ Prostaglandin synthetase inhibitors: fenamates (Mefenamic acid)
➢ Antifibrinolytic agents: Tranexamic acid
51.
• Surgical
➢ Uterinecurettage: diagnostic tool for elderly women but at times has
hemostatic and therapeutic effect by removing the necrosed and unhealthy
endometrium. It should be performed after ultrasound for detection of
endometrial pathology.
o Indication: if bleeding is acyclic and where endometrial pathology is
suspected.
o Ideally hysteroscopy and directed biopsy should be considered both for
the purpose of diagnosis and therapy.
52.
o Presently Dand C should be used neither as a diagnostic tool nor for the purpose of
therapy.
➢ Endometrial ablation/resection:
o Indications:
1. Failed medical therapy
2. Women who do not wish to preserve menstrual or reproductive
function
3. Uterus- normal size or not bigger than 10 weeks pregnancy size
4. Small uterine fibroids <3c,
5. Women who do not want surgery
6. Women who prefer to preserve their uterus
53.
Uterine artery embolization
Hysterectomy:done when conservative treatment fails or
contraindicated and blood loss impairs the health and quality of life.
Presence of endometrial hyperplasia and atypia on endometrial
histology is an indication for hysterectomy. The decision can be made
easily as the patient is approaching 40.
54.
POST-MENOPAUSAL BLEEDING
• Theis vaginal bleeding after established menopause.
➢ It is bleeding after 1 year of amenorrhea.
• All postmenopausal bleeding (PMB) must be evaluated.
• In women who are not taking cyclical Hormone replacement therapy (HRT),
any bleeding is abnormal.
• In women on combined cyclical HRT, bleeding in the progesterone free period
is normal.
• Unscheduled bleeding refers to bleeding at other times: this is abnormal and
should always be investigated
55.
ETIOLOGY
• Atrophic vaginitis(most common cause)
• Endometrial carcinoma (most common lethal cause)
• Endometrial hyperplasia
• Adenomyosis: confirmed by pathologic examination following hysterectomy
• Endometrial polyp: estrogen therapy or tamoxifen
• Cervical carcinoma (vaginal bleeding + foul smelling discharge)
• Iatrogenic anticoagulant effect
• Infection (uncommon cause of postmenopausal bleeding)
• Trauma
• Neoplasia causing PMB:
➢ Valvar and vaginal cancer, Cervical cancer: bleeding occurs as cancer outgrows its blood
supply. The necrotic and denuded tissue bleeds easily and causes a malodorous discharge (foul
smelling), Endometrial cancer, Leiomyoma of uterus, Uterine sarcoma, Fallopian tube cancer,
Estrogen secreting ovarian tumor e.g. granulosa cell tumor of the ovary.
56.
ETIOLOGY...
• The majorityof women with PMB will be found to have atrophic vaginitis,
whereby the vaginal epithelium thins and breaks down in response to low
estrogen levels. This is a benign condition, which is relatively easily treated
with topical estrogens.
• 10% of patients with PMB will have endometrial cancer, therefore all
patients
with PMB must have this diagnosis excluded promptly.
• The risk of endometrial cancer progressively increases with age
57.
HISTORY AND EXAMINATION
•Initial step is to establish that it is vaginal bleeding and not bleeding per rectum or hematuria.
• History
➢ When was your last period (i.e. confirm age of menopause)
➢ Menstrual pattern prior to menopause
➢ Ask the patient about the frequency, duration and amount of bleeding and when it was first noticed.
➢ Ask the patient about any associated signs/symptoms like weight loss, fever
➢ History of trauma
➢ Was the bleeding post-coital (i.e. think cervical polyp/cervical malignancy)
➢ Sensation of something coming out of the introitus.
➢ Urinary problems like dysuria or frequency of urination
➢ When was your last smear done? Have they always been normal (i.e. think cervical malignancy)
➢ Ask the patient which medications she takes- hormones (estrogen), anticoagulants, tamoxifen, over the
counter, herbal supplements
➢ Ask about the past medical history
➢ Family history of bleeding, gynecologic cancer, breast cancer (first degree relative)
58.
Examination
• Examination shouldinclude an abdominal and vaginal examination to
detect
any pelvic masses and a speculum to visualize the vaginal tissues for atrophy
and the cervix for polyps or potential carcinoma.
➢ Note any suspicious lesions, lacerations, discharge or foreign bodies.
➢ Classic signs of atrophy include pale, dry vaginal epithelium that has lost
its rugae
➢ Assess the size, contour and tenderness of the uterus
• A smear should be taken if due
59.
INVESTIGATIONS
• An ultrasoundscan should be carried out in all women to assess endometrial
thickness.
➢ If thickness is 3mm or less (or 5mm or less for women of HRT) patients can be
reassured that the likelihood for endometrial carcinoma is extremely
low and no further investigation is required.
➢ For those with an endometrial thickness >3mm (5mm for those on HRT) further
endometrial assessment is warranted in the form of an endometrial biopsy.
➢ Exception: is women on tamoxifen as ultrasound will not assist with a diagnosis.
Most women on tamoxifen will have a thickened, irregular and cystic
endometrium. Immediate direct visualization of the cavity by hysteroscopy and an
endometrial biopsy is the investigation of choice for such women.
60.
• Endometrial canceris most prevalent in the post-menopausal age group.
➢ It typically presents with PMB
➢ Risk factors; Nulliparity, Obesity, Early menarche, Late menopause,
Tamoxifen exposure.
➢ Diagnosis is by endometrial biopsy
➢ Endometrial cancer treatment should begin with staging which involves
total abdominal hysterectomy with washings, bilateral
salpingo_x0002_oophorectomy and lymph node evaluation
➢ The need for postoperative adjuvant radiotherapy is determined by
recurrence risk.
61.
• Pap smearfor cervical dysplasia, neoplasia.
• Diagnostic dilation and curettage
• Hysteroscopy
62.
MANAGEMENT
• Atrophic vaginitis:topical estrogen cream, estrogen pessaries or estrogen ring
pessary
• Cervical polyp: remove via speculum examination using polyp forceps
• Endometrial polyp: remove under direct visualization at hysteroscopy
• Simple hyperplasia: progestogens (oral preparation or LNG-IUS-Mirena)
• Complex hyperplasia: Progestogens (oral preparations of LNG-IUS-Mirena)
• Atypical hyperplasia: total abdominal hysterectomy as significant risk of
progression to malignancy
• Endometrial cancer: total abdominal hysterectomy + bilateral
salpingo_x0002_oophrectomy + washings +/- adjuvant therapy