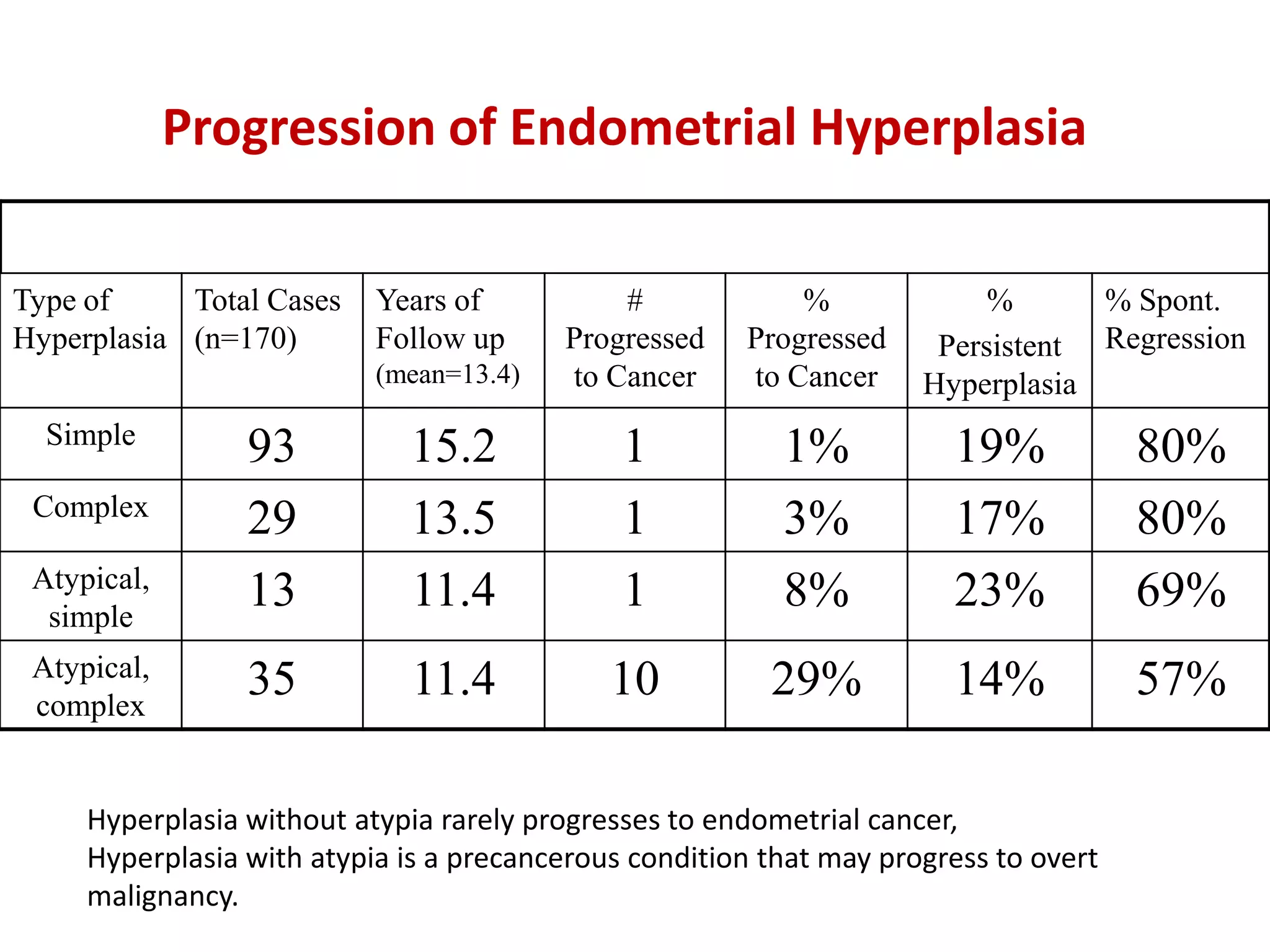
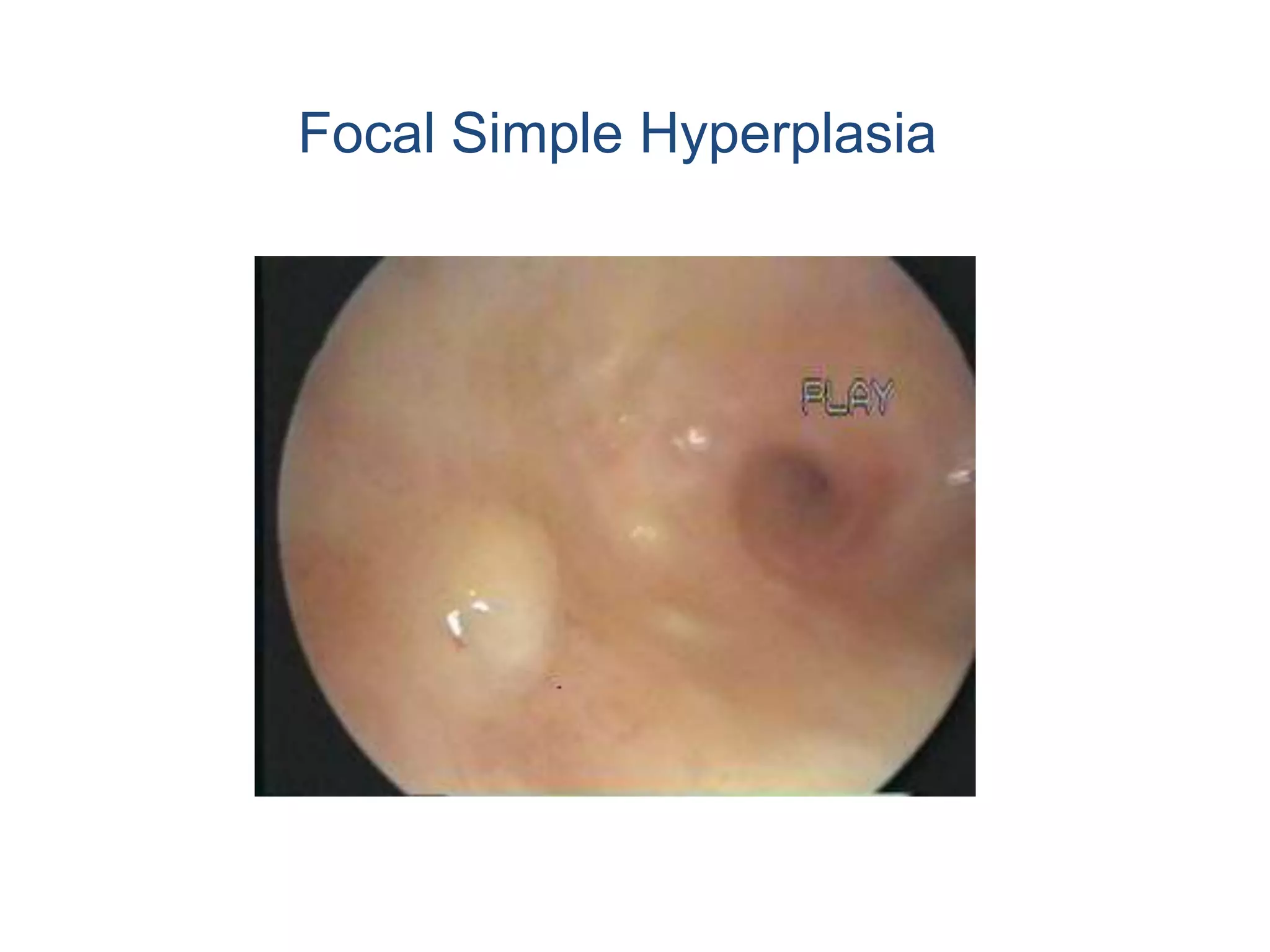
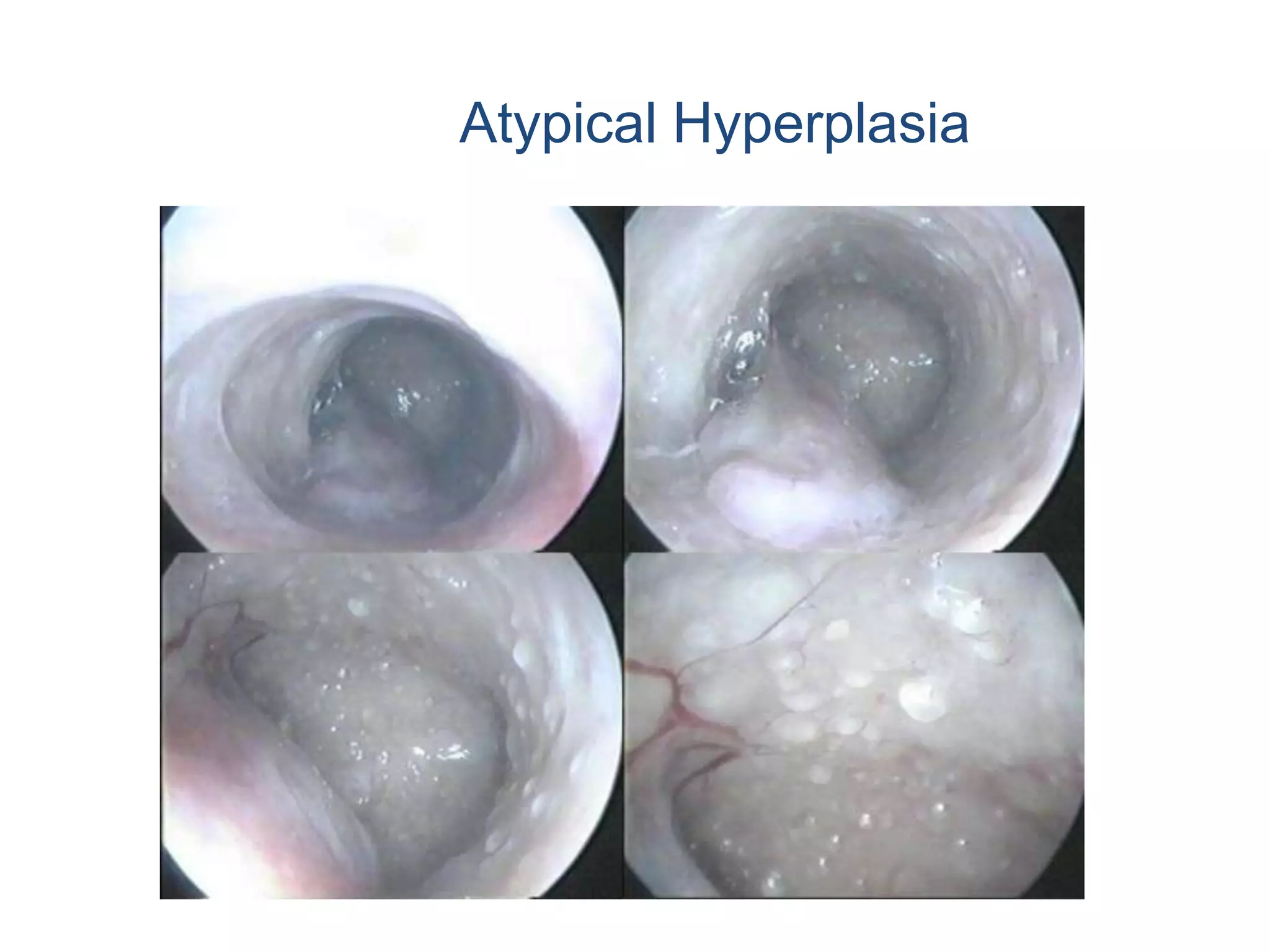
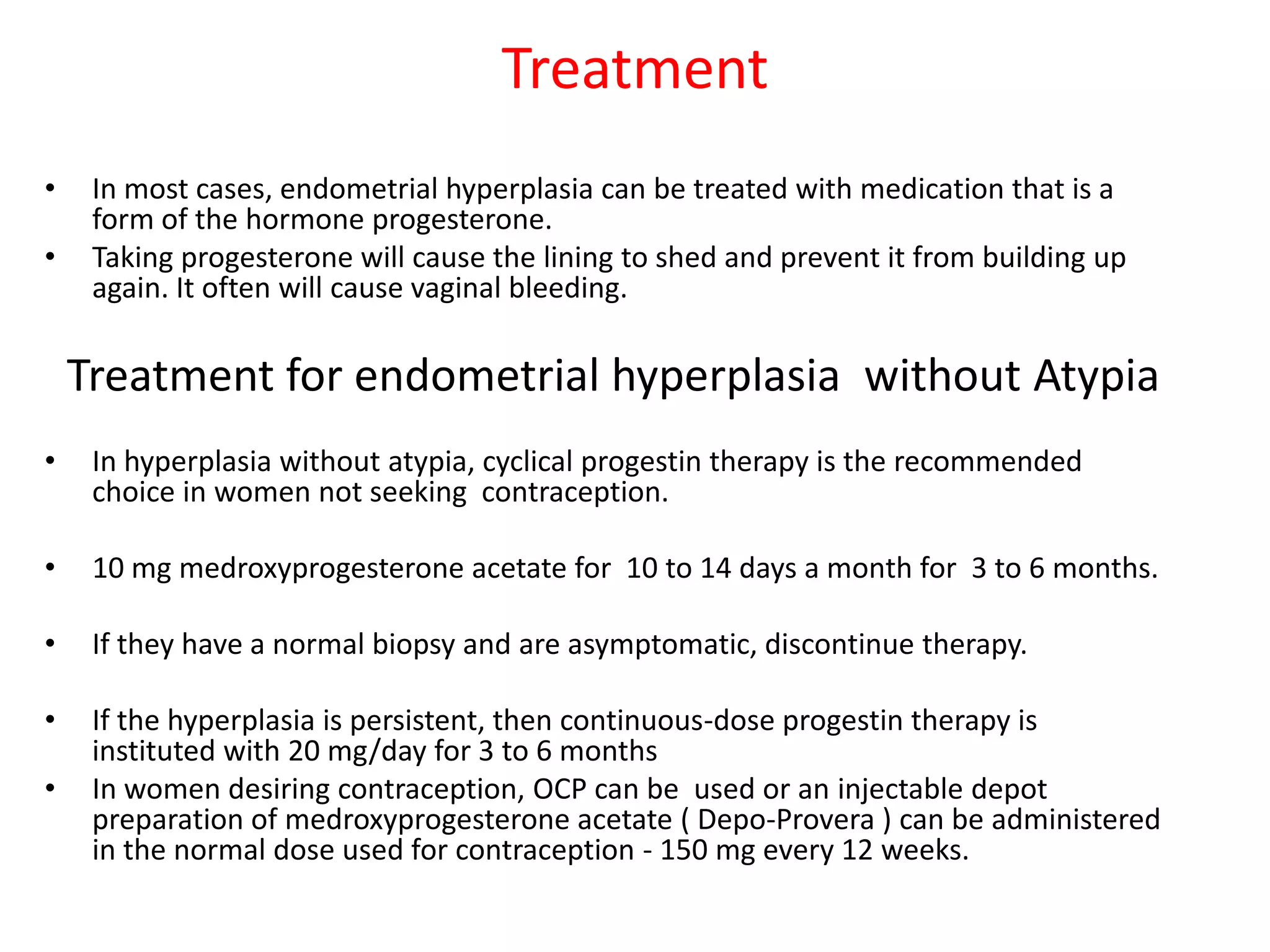
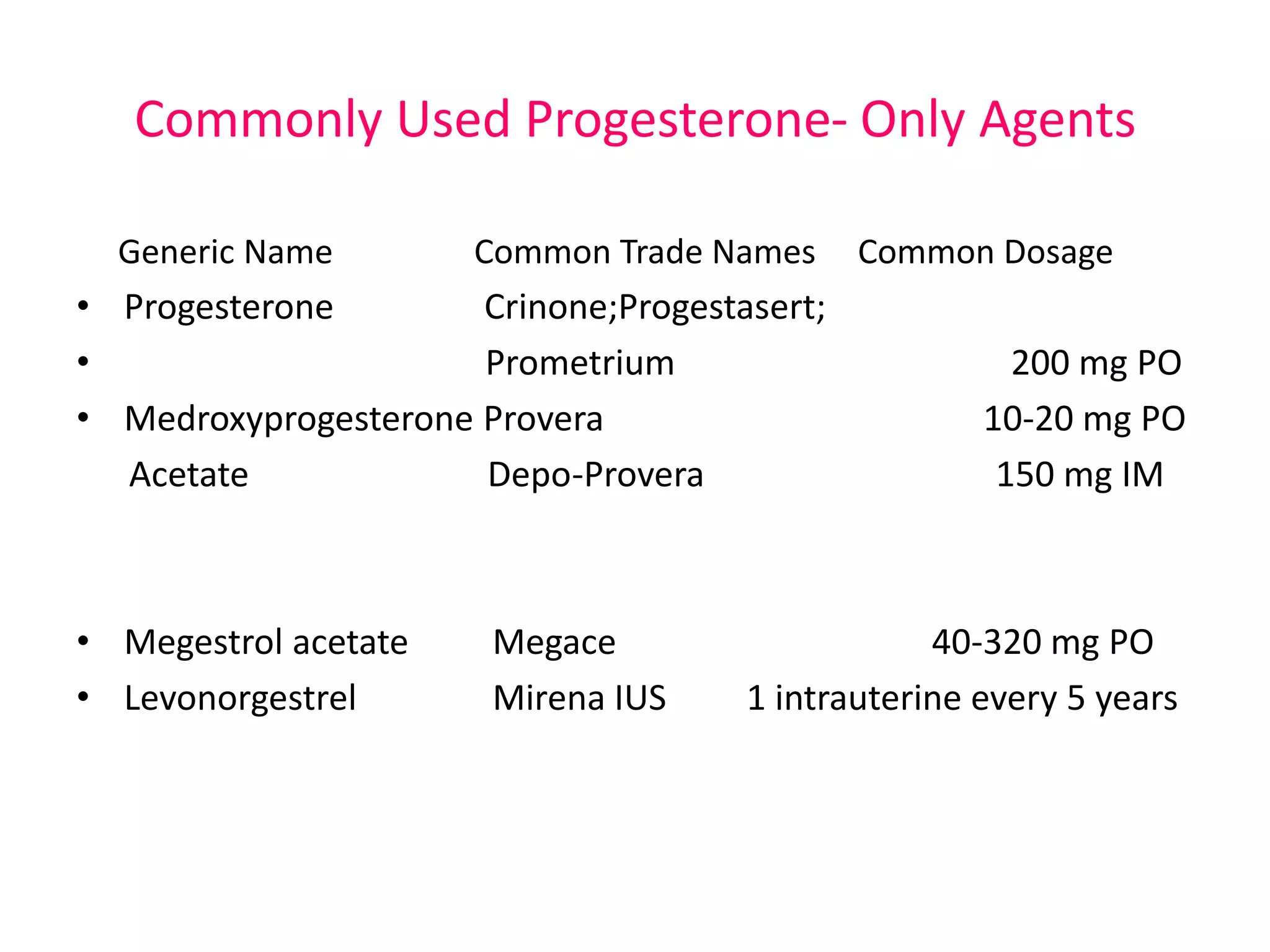
Endometrial hyperplasia is a non-cancerous condition where the cells of the endometrium proliferate excessively. It occurs when the endometrium is exposed to unopposed estrogen due to lack of progesterone. There are different classifications of hyperplasia from simple to complex and atypical. Atypical hyperplasia is a precancerous condition. Symptoms include abnormal bleeding. Treatment involves taking progesterone medications to shed the endometrial lining. For atypical hyperplasia, hormonal therapy or hysterectomy may be needed due to high cancer risk. Preventing excess estrogen exposure can reduce hyperplasia risk.