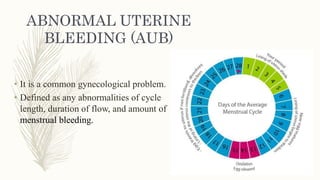
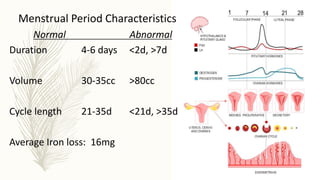
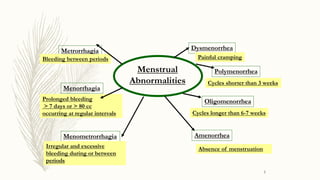
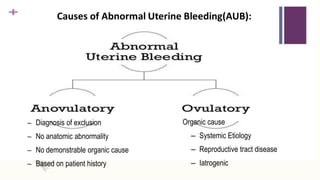
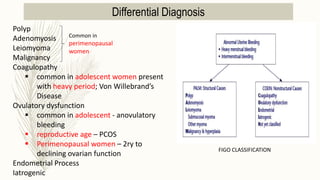
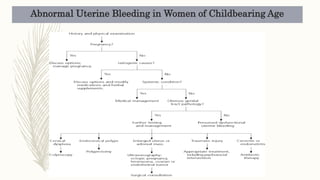
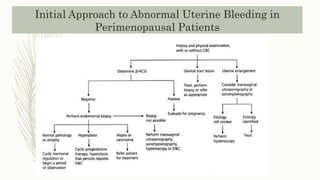
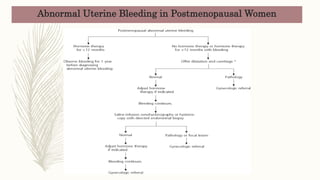
This document discusses abnormal uterine bleeding (AUB), which is defined as any abnormalities in menstrual cycle length, flow duration, or amount. It provides details on the types of AUB, causes by age group, evaluation, differential diagnosis, and management. The main types of AUB include amenorrhea, dysmenorrhea, menorrhagia, oligomenorrhea, and metrorrhagia. Causes can be organic lesions, anovulatory cycles, coagulation disorders, or dysfunctional uterine bleeding. Evaluation involves history, exam, lab tests like CBC and imaging. Management options include general measures, medical treatment with hormones or intrauterine devices, and surgical intervention if needed.