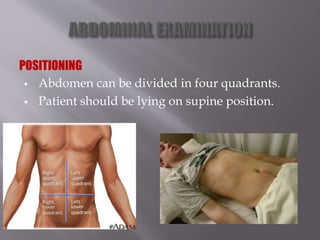
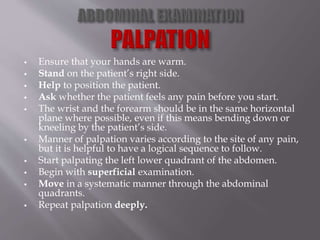
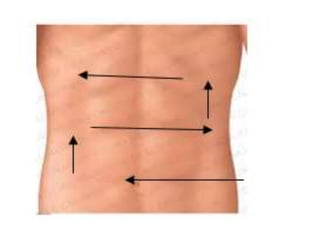
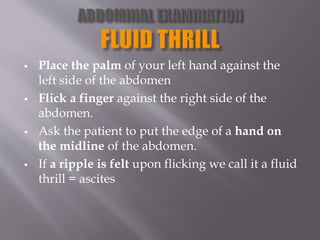
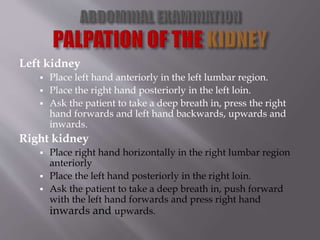
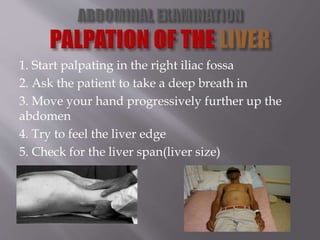
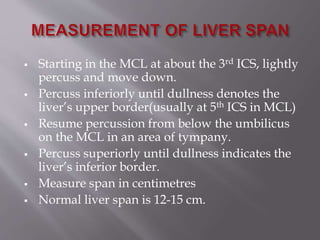
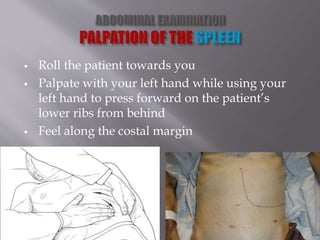
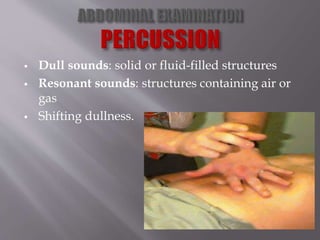
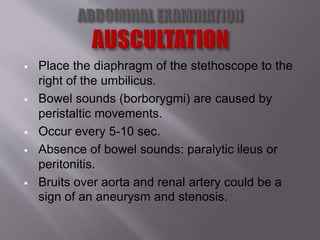
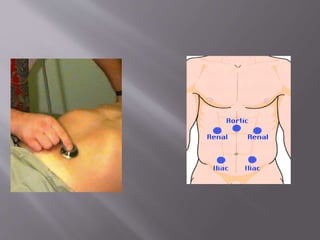
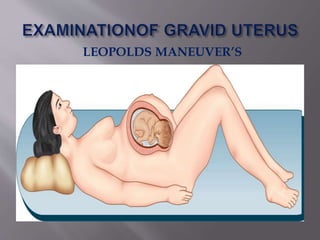
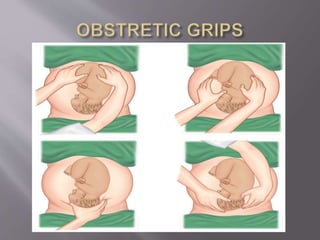
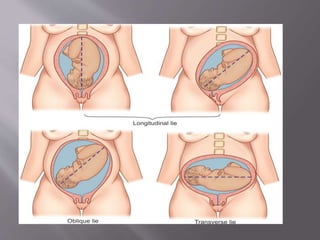
This document provides guidance on performing an abdominal examination including inspection, palpation, percussion, and auscultation. It describes examining the abdomen systematically by quadrant and outlines key points for palpating each region. Specific assessments are described such as rebound tenderness to check for peritonitis. The document also covers examining the liver, kidneys, and gravid uterus along with maneuvers like Pawlik's grip and Leopold's.
































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





