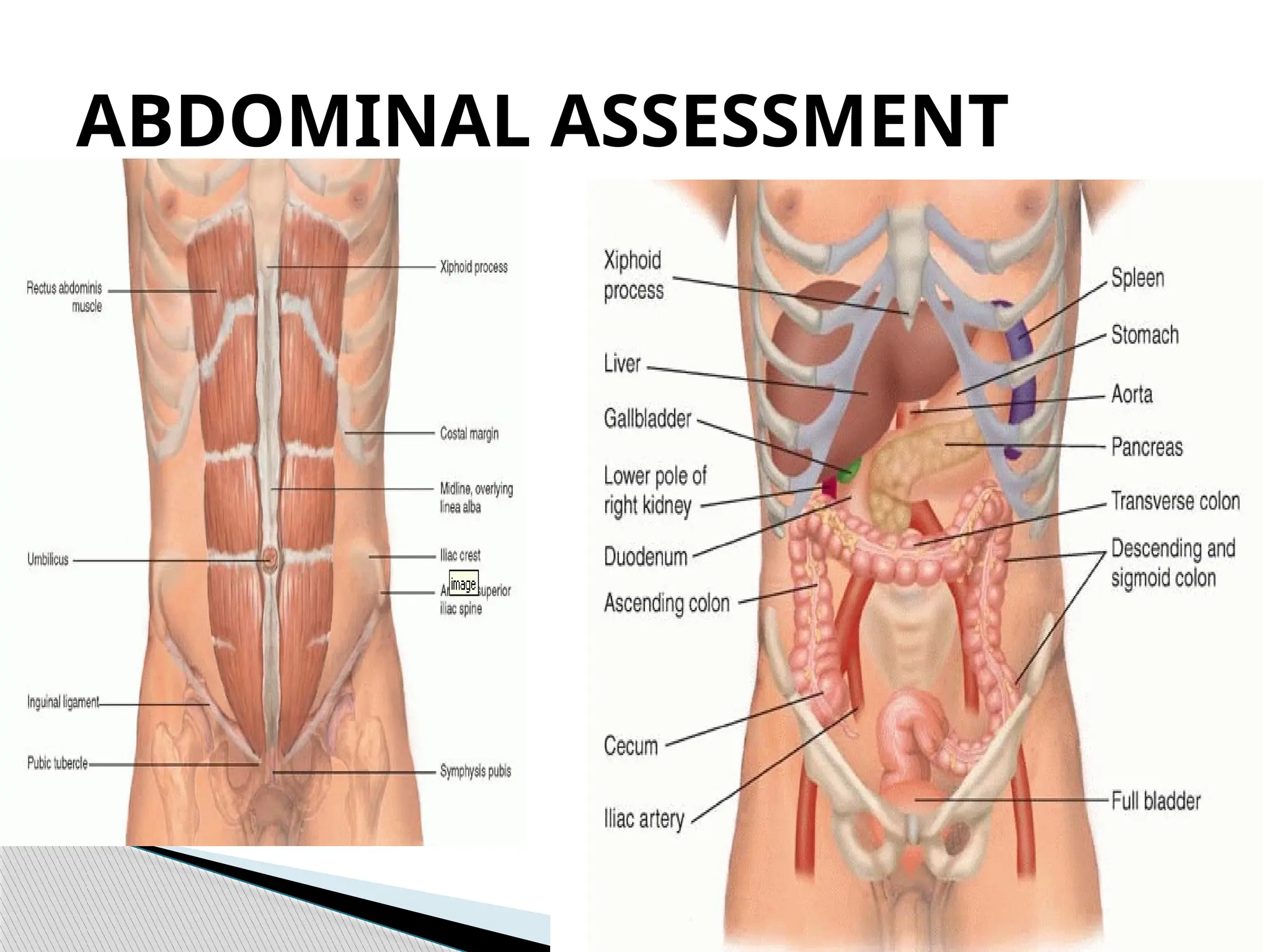
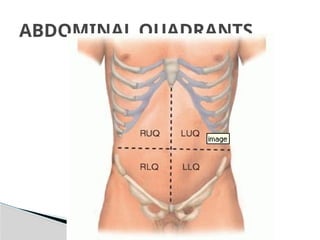
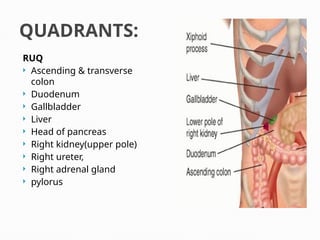
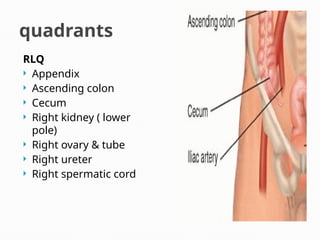
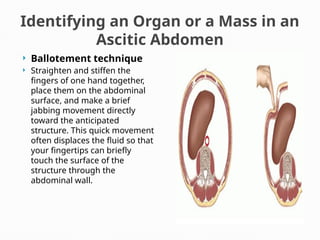
The document outlines a comprehensive approach to abdominal assessment, detailing the anatomical regions, examination techniques, and indications for various conditions related to abdominal pain. It includes descriptions of palpation techniques, auscultation methods, and specific tests for conditions like ascites and appendicitis. The text emphasizes the importance of patient positioning, comfort, and systematic examination to ensure accurate diagnosis.