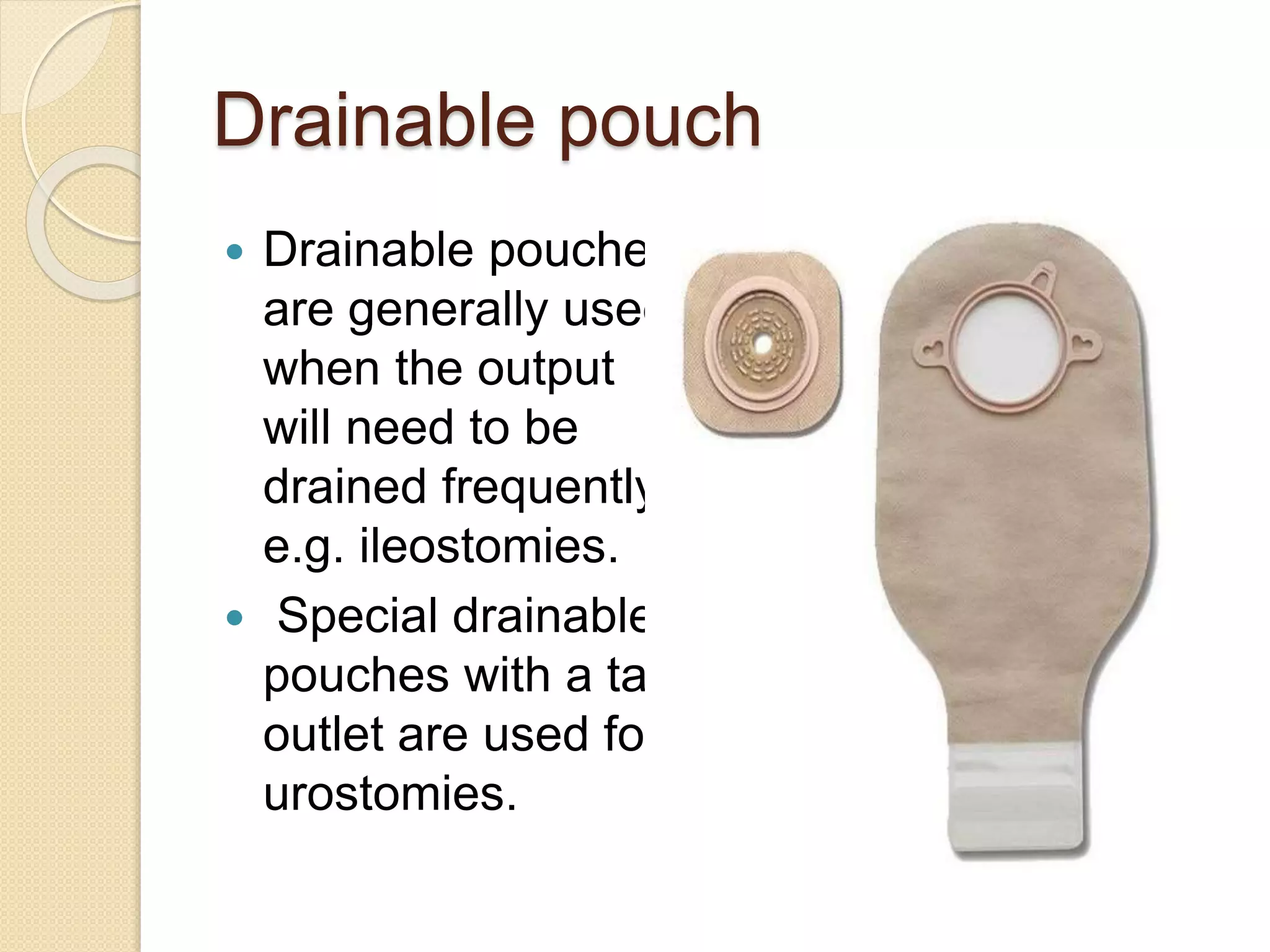
The document discusses different types of intestinal ostomies including colostomies. It describes the procedure for colostomy care including necessary supplies, assessment of the stoma, cleaning and changing the pouch and barrier. Guidelines are provided such as checking the stoma regularly, keeping the skin clean and dry, and recording intake and output. Drainable pouches are used when frequent emptying is needed and one-piece or two-piece pouches can be used.