


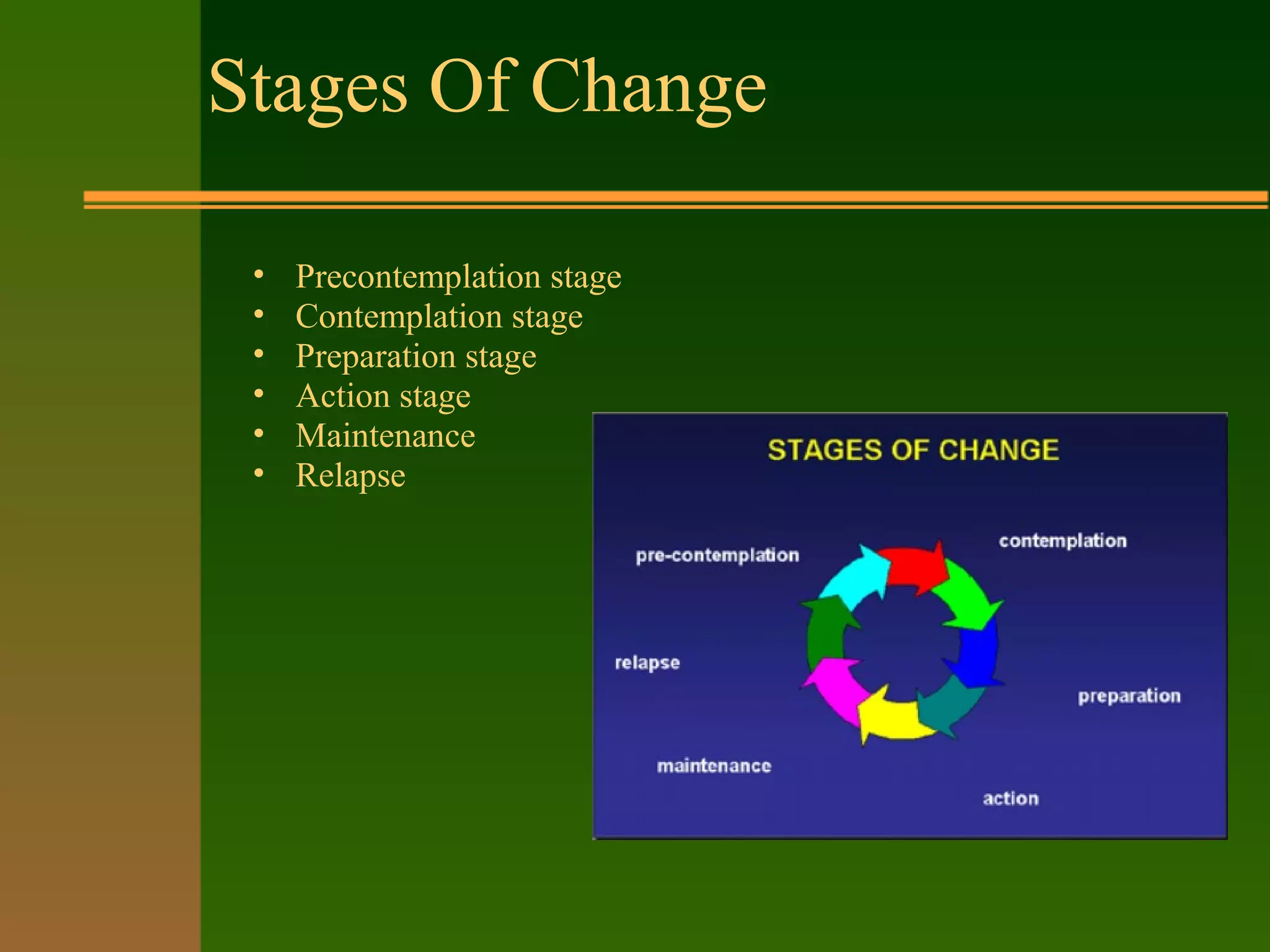


This document provides an overview of enhancing motivation to change among substance-using adolescents. It discusses the challenges adolescents face at home that could contribute to drug use. Motivation is presented as fluid rather than a fixed trait. Motivational interviewing is outlined as an effective approach that minimizes resistance by accepting different stages of change. The stages of change are defined as precontemplation, contemplation, preparation, action, maintenance, and relapse. Clinical strategies are suggested for each stage, such as raising doubts in precontemplation and helping resolve ambivalence in contemplation.























































































