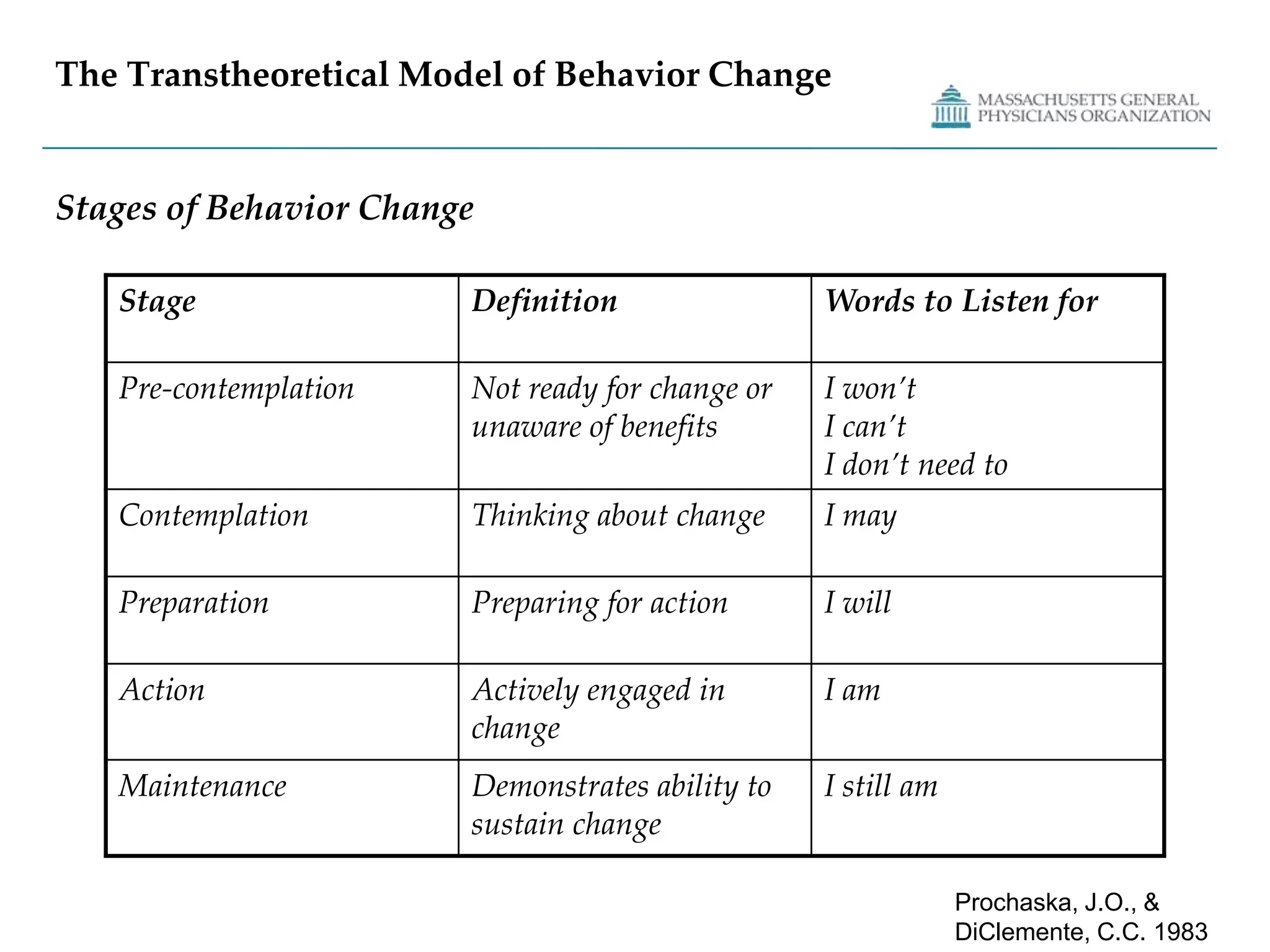
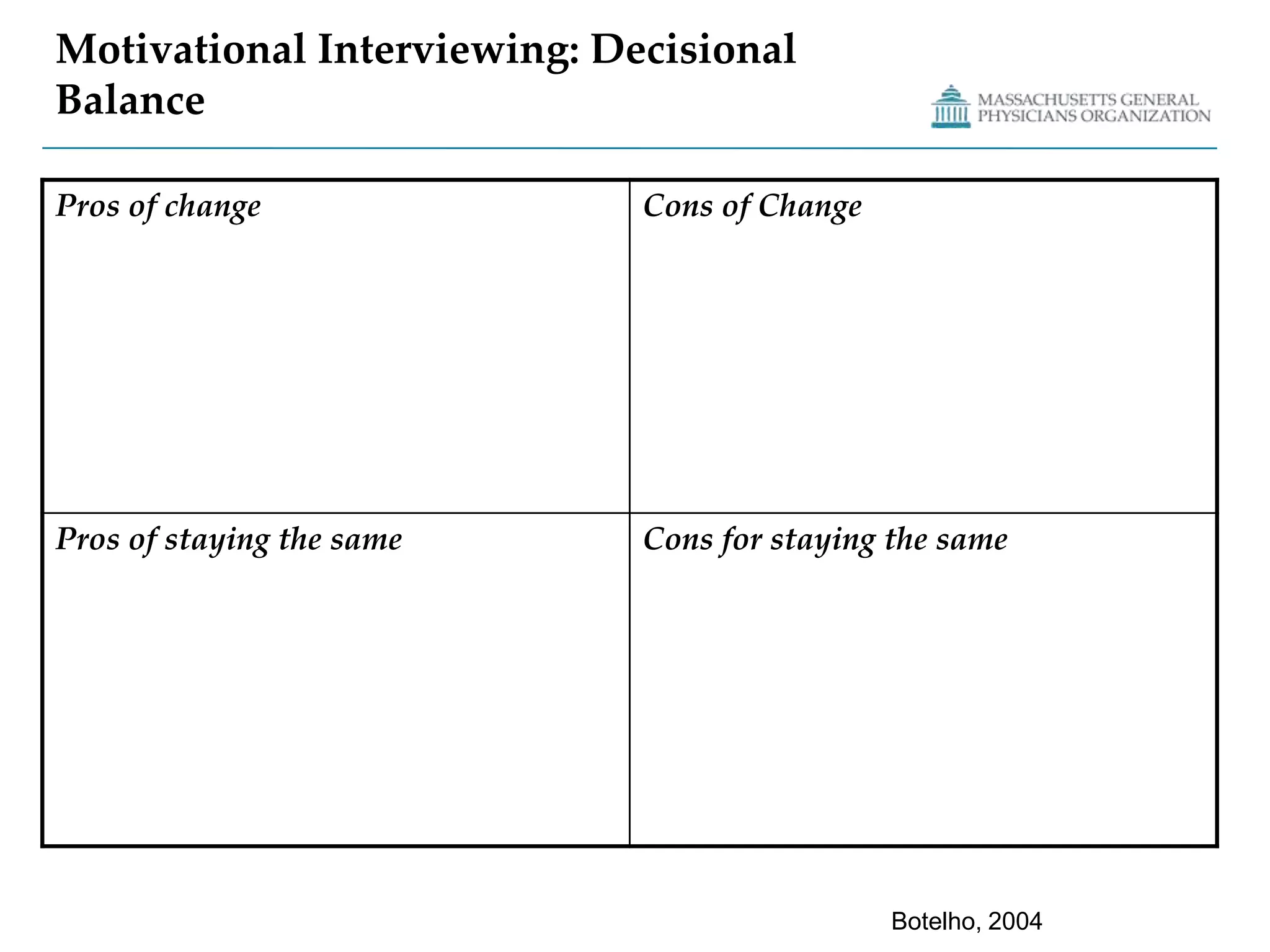
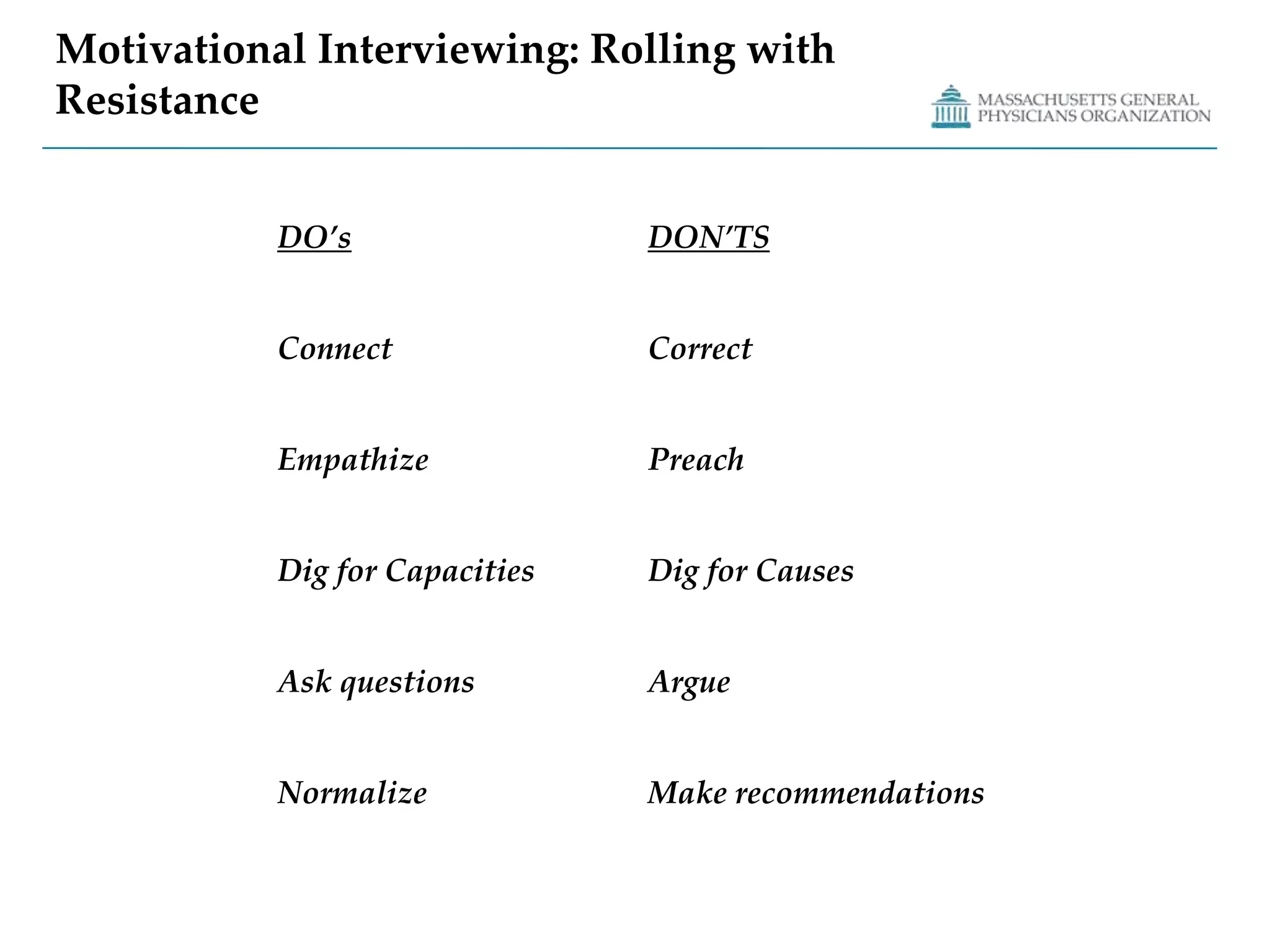
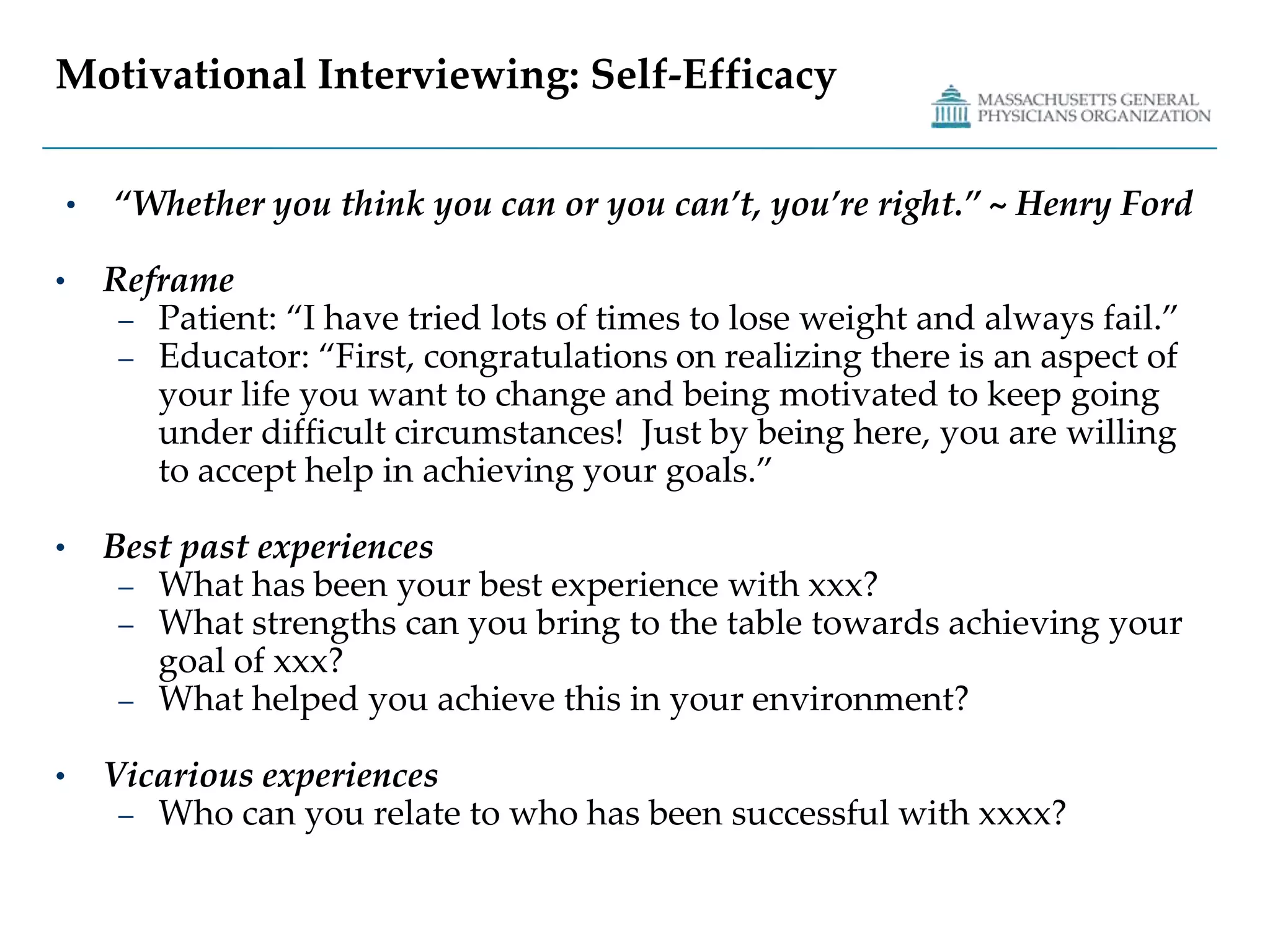
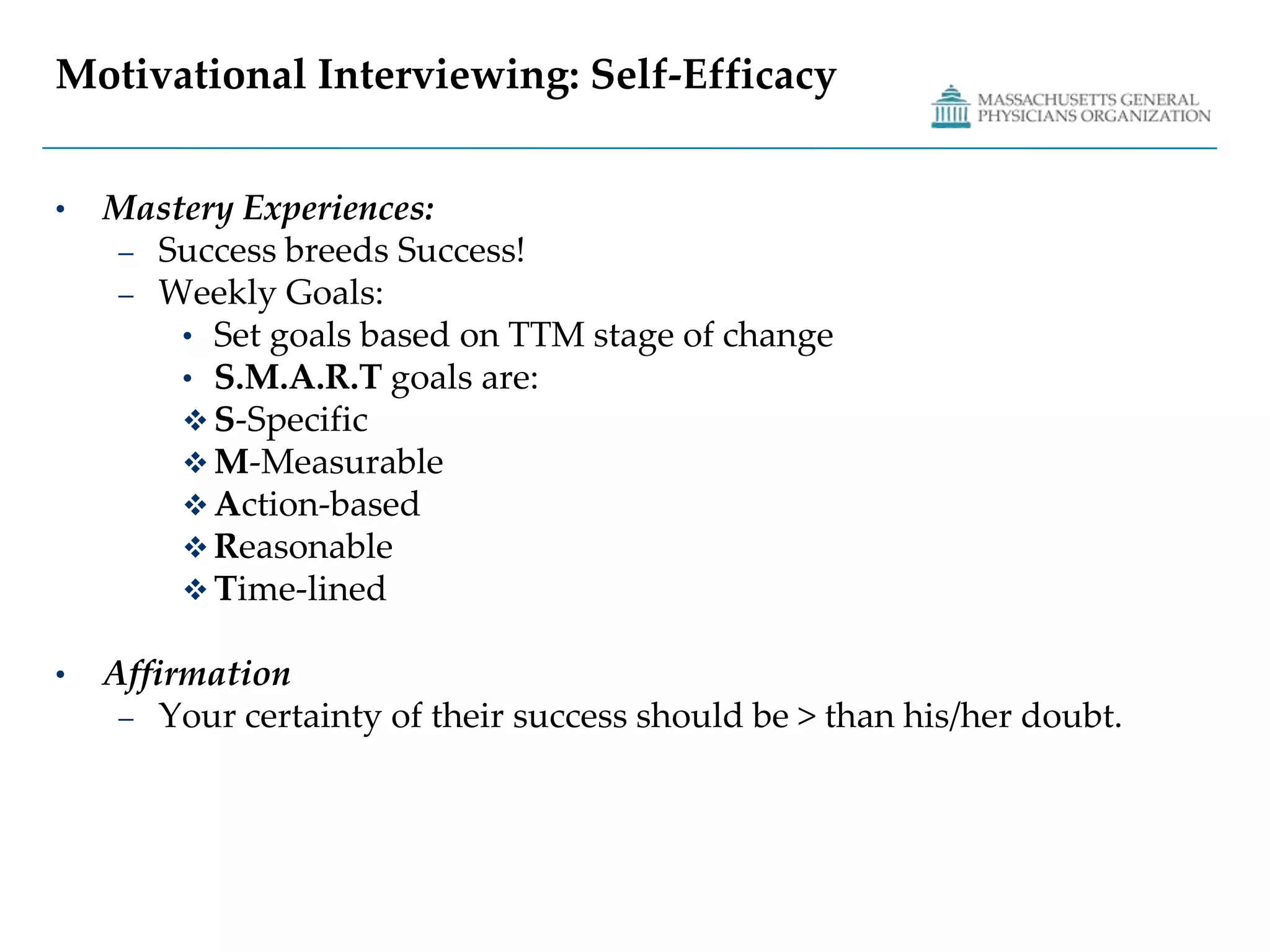
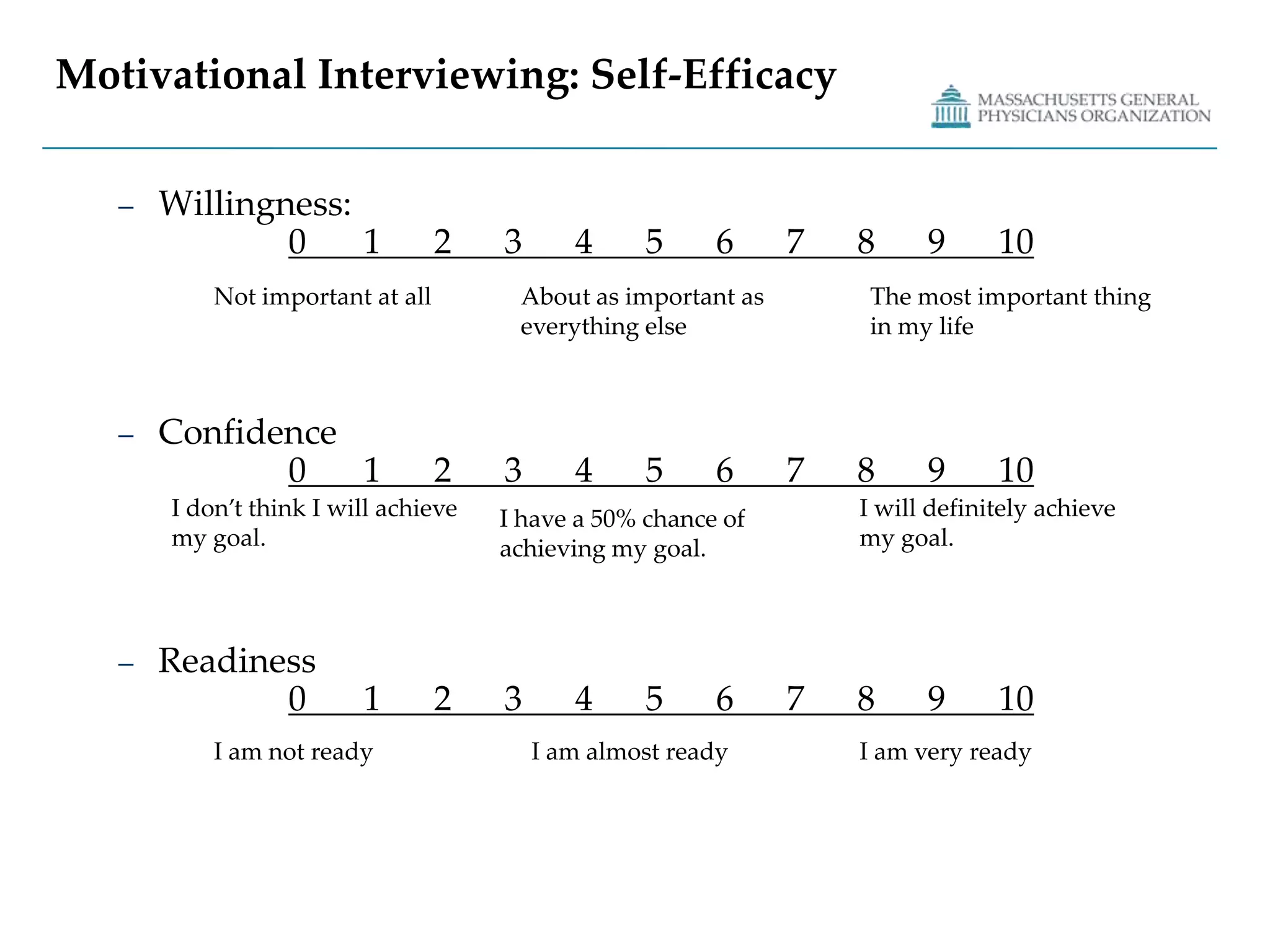
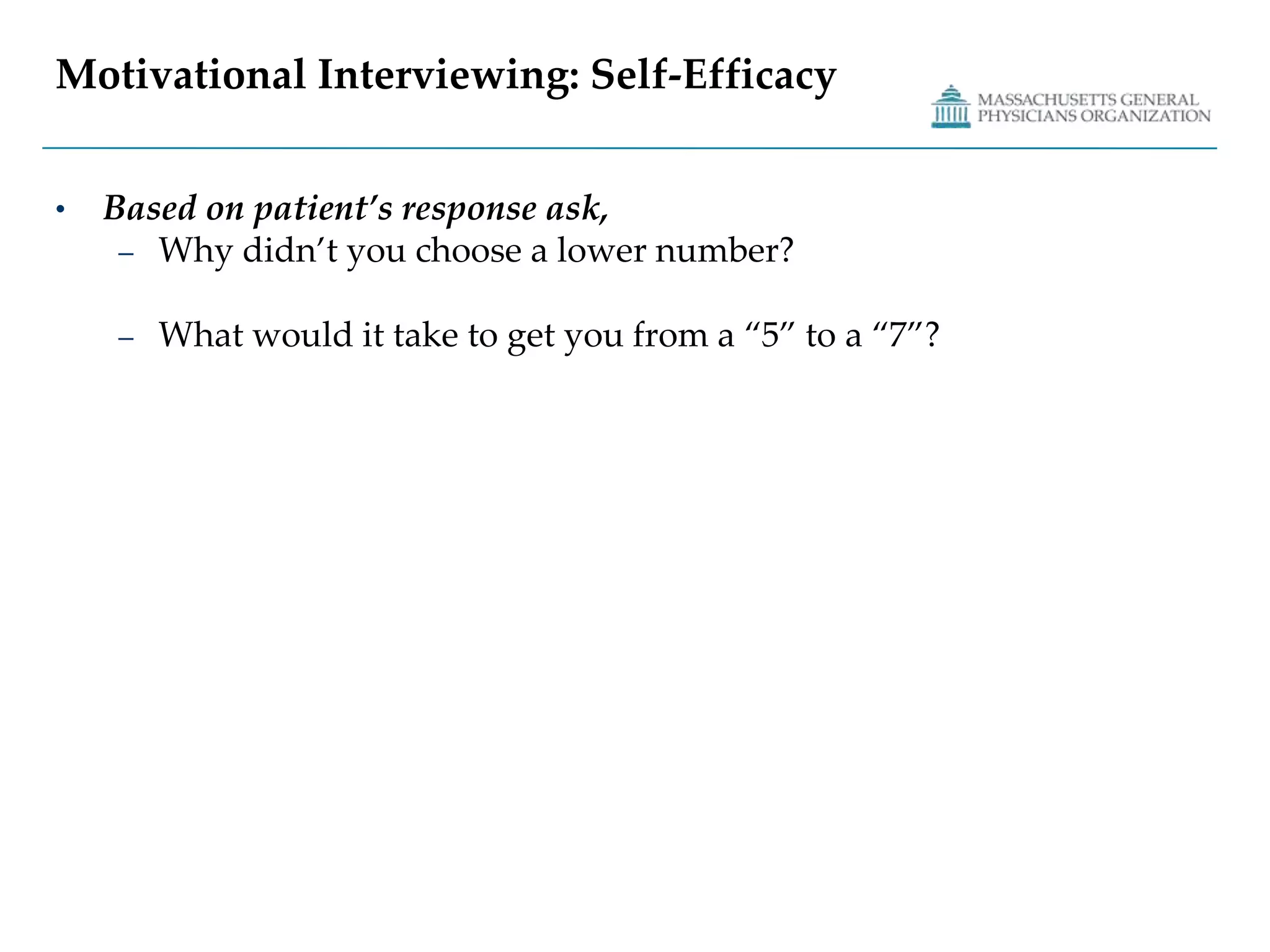
The document summarizes the Transtheoretical Model of Behavior Change and Motivational Interviewing. It discusses the five stages of behavior change according to the Transtheoretical Model and the 10 processes of progressing through the stages. It then defines Motivational Interviewing and describes its patient-centered skills, styles, and strategies to promote behavior change from within. The guiding principles of Motivational Interviewing involve expressing empathy, avoiding argument, developing discrepancy, rolling with resistance, and supporting self-efficacy.