Downloaded 66 times
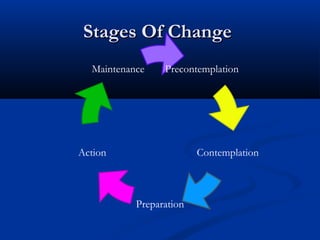

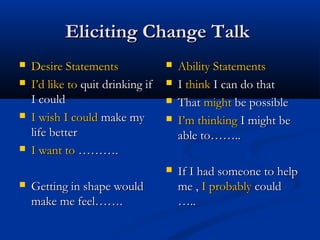
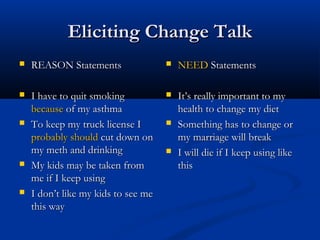
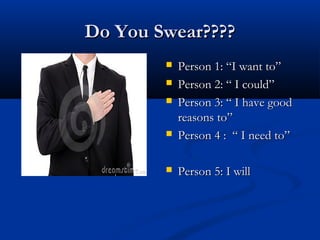
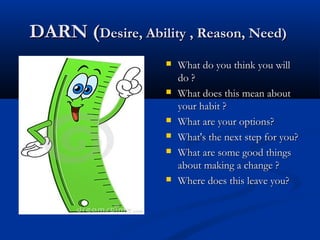

The document discusses motivational interviewing (MI), a client-centered counseling approach designed to elicit behavior change by helping clients explore and resolve their ambivalence. It details the stages of change and the counselor's role in facilitating transitions through each stage, as well as providing practical strategies for expressing empathy, developing discrepancies, and rolling with resistance. Various exercises and pitfalls in the counseling process are described to enhance the effectiveness of the MI approach.











































































































