Downloaded 200 times
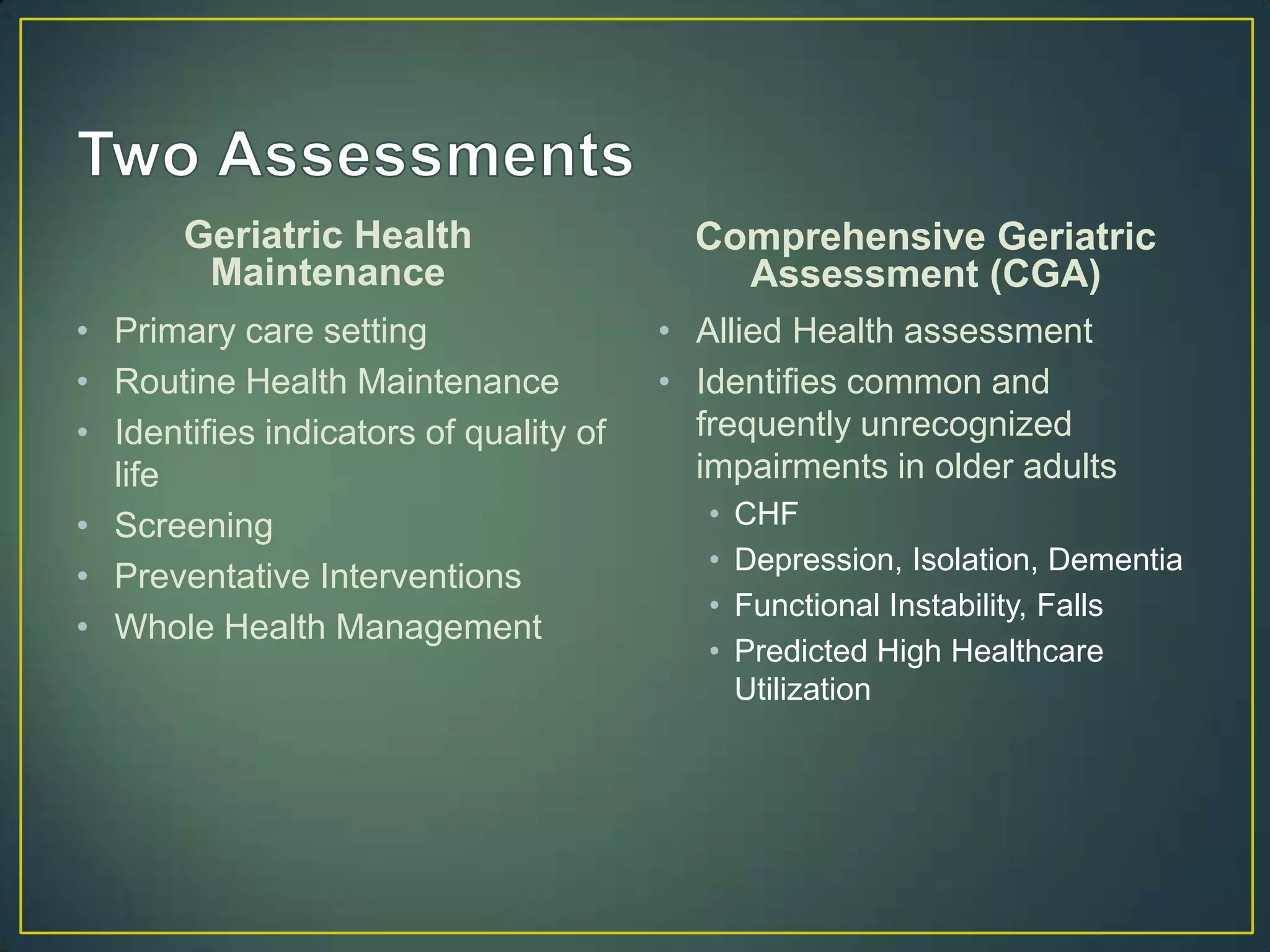

















The document discusses geriatric health maintenance and comprehensive geriatric assessments. It outlines the components of primary, secondary, and tertiary prevention for older adults, including screening tests, immunizations, and identifying/managing common conditions like falls, incontinence, and medication management. Comprehensive geriatric assessments evaluate multiple domains like function, cognition, mood, social support and goals of care to develop care plans for older patients.


































































