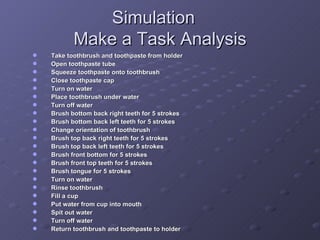
The document discusses terminology, definitions, prevalence, causes, identification and assessment, characteristics, and educational considerations for students with severe disabilities including severe intellectual disabilities, multiple disabilities, deaf-blindness, physical disabilities such as orthopedic impairments and other health impairments, and traumatic brain injury. It provides definitions from IDEA and discusses the complex nature of identifying and assessing students with multiple, co-occurring disabilities that affect cognitive, physical, sensory, and behavioral functioning.







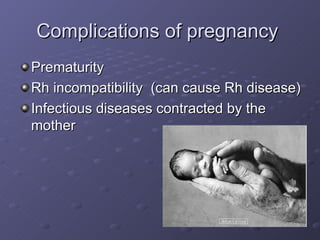

![IDEA states: “…‘ children with severe disabilities’ refers to children with disabilities who, because of the intensity of their physical, mental, or emotional problems, need highly specialized education, social, psychological and medical services…autism, severe and profound mental retardation, and those who have two or more serious disabilities such as deaf-blindness, mental retardation and blindness, and cerebral palsy and deafness. They may also have…“severe speech, language, and/or perceptual-cognitive deprivations and evidence of abnormal behavior such as failure to respond to pronounced social stimuli, self-mutilation, self-stimulation, manifestation of intense and prolonged temper tantrums, and the absence of rudimentary forms of verbal control; and may also have extremely fragile psychological conditions.” (34 C.F.R., Sec. 315.4[d]) (pp. 470 of textbook)](https://image.slidesharecdn.com/GROUPdraftMultipleDisabilitiesPresentation-122803661756-phpapp02/85/Group-Draft-Multiple-Disabilities-Presentation-38-320.jpg)






























![Multiple Disabilities[1] Copy](https://cdn.slidesharecdn.com/ss_thumbnails/multiple-disabilities1-copy-1229371984968951-2-thumbnail.jpg?width=640&height=640&fit=bounds)































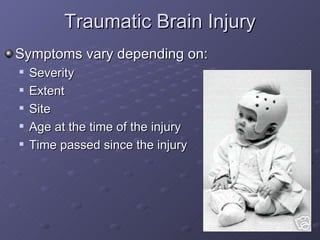
![Traumatic brain injury[2]](https://cdn.slidesharecdn.com/ss_thumbnails/traumaticbraininjury2-101201203940-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






