CPDA BLOOD BAG
• SPECIFICATIONS
• Primary Bag capacity available in 150ml to 500ml
• Donor needle gauge size: 16G to 17G
• Package: Each set packed in one compounded
vacuum pouch
6.
CPDA BLOOD BAG
OPTIONALFEATURES
• Attached Blood Sampling Bag
• Needle Protector
• Tube Holder
• "Y" injection port
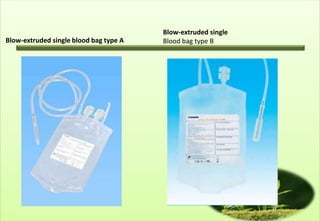
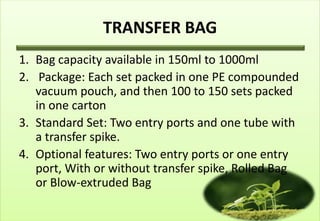
TRANSFER BAG
1. Bagcapacity available in 150ml to 1000ml
2. Package: Each set packed in one PE compounded
vacuum pouch, and then 100 to 150 sets packed
in one carton
3. Standard Set: Two entry ports and one tube with
a transfer spike.
4. Optional features: Two entry ports or one entry
port, With or without transfer spike, Rolled Bag
or Blow-extruded Bag
Transfusion
• Blood Transfusionbecome availabe in 1829
• Now a days no severe reactions to transfusion
seen.
• Immunosuppresion to host occurs.
11.
Blood & BloodProducts
• Donated Blood are leucodepleted as a precaution
against creutzfeldt-Jakob Diseases (transmissible
spongiform encephalopathies )
Packed red cells
•Packed red blood cells are cells that are spun
down and concentrated. Each unit is
approximately 330ml and has a haematocrit of 50-
70%. Packed cells are stored in a SAG-M solution
(Saline-adenine-glucose-mannitol)to increase their
shelf-life to 5 weeks at 2-60C. (Older storage
regimens included storage in CPD – citrate-
Phosphate-dextrose solutions –giving cells a shelf-
life of 2-3 weeks).
14.
Fresh Frozen Plasma
FFPis rich in coagulation factors
• It is removed from fresh blood and stored at -40
to 50 0C with a 2 year shelf life.
• It is the first line therapy in the treatment of
coagulopathic haemorrhage.
• Rhesus D positive FFP may be given to a Rhesus D
negative woman
15.
Cryoprecipitate
• Cryoprecipitate isa supernatant precipitate of FFp
and is rich In factor VIII and fibrinogen.
• It is stored at -30oC with a 2 year shelf life.
• It is given in low fibrinogen states or in cases of
factor VIII deficiency.
16.
Platelets
• Platelets aresupplied as a pooled platelet
concentrate containing about 250×109 cells per
litre.
• Platelets are stored on a special agitator at 20-240
C and have a shelf life of only 5 days
• Platelets Transfusions are given to patients with
thrombocycopenia.
17.
Prothrombin Complex Concentrates
•Prothrombin complex concentrates (PCCs) are
highly purified concentrates prepared frompooled
plasma.
• They contain factors II,IX and X; factor VII may be
included or produced seperately.
• PCCs are indicated for the emergency reversal of
anti- coagulant (warfarin) therapy in uncontrolled
haemorrhage.
18.
Autologous blood
• Predonation of their own blood patients
undergoing elective surgery up to 3 weeks surgery
of retransfusion.
• Collected in a cell saver, ( which washes and
collects red blood cells) which can then be
returned to the patient.
19.
Indication of bloodTransfusion
• Acute blood loss, to replace circulating volume
and maintain oxygen delivery
• Perioperative anaemia, to ensure adequate
oxygen delivery during to perioperative phase
• Symptomatic chronic anaemia without
hemorrhage or impending surgery.
20.
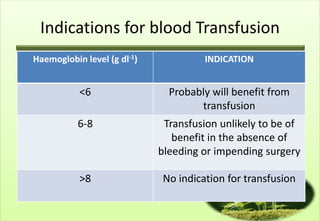
Indications for bloodTransfusion
Haemoglobin level (g dl-1) INDICATION
<6 Probably will benefit from
transfusion
6-8 Transfusion unlikely to be of
benefit in the absence of
bleeding or impending surgery
>8 No indication for transfusion
21.
Blood Groups andCross Matching
• ABO System
– The system consists of 3 allelic genes A, B & O.
– Control the synthesis of enzymes that add
carbohydrate residues to cell surface glycoproteins
– A & B genes result in specific residues
– The O gene is an amorph & doesn’t transform the
glycoprotein.
– The system allows for six possible genotypes although
there are four phenotypes.
22.
ABO blood groupSystem
Phenotype Genotype Antigen Antibodies Frequency (%)
O OO O Anti-A, Anti-B 46
A AA or AO A Anti-B 42
B BB or BO B Anti-A 9
AB AB AB None 3
Rhesus System
The Rhesus D [Rh(D)] antigen is strongly antigenic.
Antibodies to the D antigen are not naturally present in the serum of the
remaining 15% of individuals but their formation may be stimulated by the
transfusion of Rh-positive red cells or they may be acquired during delivery of
a Rh(D) positive baby.
23.
TRANSFUSION REACTIONS
• isany unfavorable transfusion-related event occurring in a
patient during or after transfusion of blood components
24.
TRANSFUSION REACTIONS
@RBC’s !
•Nonhemolytic 1-5 % transfusions
Causes -Physical or chemical destruction of
blood: freezing, heating, hemolytic drug
-solution added to blood
-Bacterial contamination
: fever, chills, urticaria
– Slow transfusion, diphenhydramine , antipyretic for fever
• Hemolytic
– Immediate: ABO incompatibility (1/ 12-33,000) with fatality (1/ 500-800,000)
Majority are group O patients receiving
type A, B or AB blood Complement activation,
RBC lysis, free Hb (+ direct Coombs Ab test)
25.
Cross Matching
• Fullcross matching of blood takes 45 min in most
laboratories.
• In more urgent situations, “type-specific” blood is
provided can be issued within 10-15 min.
• When blood must be given in an emergency,
group O (Universal donor) blood is given (O- to
female patients, O+ to male patients)
26.
Complications of bloodTransfusion
• From a Single Transfusion
– Incompatibility haemolytic transfusion reaction
– Febrile transfusion reaction
– Allergic reaction
– Infection
• Bacterial infection (usually as a result of faculty storage)
• Hepatitis
• HIV
• Malaria
– Air embolism
– Thrombophylebitis
– Transfusion related acute lung injury (usually from FFP)
27.
Complications of bloodTransfusion
• From Massive Transfusion
– Coagulopathy
– Hypocalcaemia
– Hyperkalaemia
– Hypokalaemia
– Hypothermia
Patient who receive repeated transfusions e.g
Patient with thalessaemia may develop iron
overload
28.
Management of Coagulopathy
•Standard Guidelines
– FFP if prothrombin time (PT) or partial Thromboplastin
time (PTT) > 1.5 × normal
– Cryoprecipitate if fibrinogen < 0.8 gl-1
– Platelets if platelet count < 50 × 109 ml-1
29.
Blood Substitutes
• Bloodsubstitutes are either biomimetic or abiotic
– Biomimetic substitutes mimic the standard oxygen-
carrying capacity of the blood and are haemoglobin
based
– Abiotic substutes are synthetic oxygen carriers and are
currently primarily per fluorocarbon based.
30.
Plasma Expanders
• Dextran is a complex,
branched glucan (polysaccharide made of
many glucose molecules) composed of chains of
varying lengths (from 3 to 2000 kilodaltons). It is
used medicinally as an antithrombotic (anti-
platelet), to reduce blood viscosity, and as a
volume expander in anemia.
31.
“Blood is stillthe best possible thing to have in our
veins” - Woody Allen
Blood transfusion is a lot like marriage.
It should not be entered upon lightly, unadvisedly or wantonly,
or more often than is absolutely necessary” - Beal
Questions & Comments
1. CPDA bags
a. Blood storage bags.
b. Urine storage bags.
c. Its saline storage bags
d. Its coffee storage bags
e. Not always sterile
34.
Questions & Comments
2.Following are the true statements about types of
blood available for transfusion
a. Whole blood
b. Packed red cells
c. Fresh frozen plasma (FFP)
d. Autologous blood
e. Blood stored more than 6 months
35.
Questions & Comments
3.Following are true about FFP
a. Rich in coagulation factor
b. Remove from fresh blood
c. Stored at -40 to 500 C
d. It is first line treatment of coagulapathic
haemorrhage
e. It can be used even after 4 years
36.
Questions & Comments
4.Autologous blood is
a. Blood from other individual
b. Blood from same individual taken from 1 vein &
given through the other vein.
c. Its blood taken 3 weeks before surgery from the
same patient for the re transfusion
d. Its blood collected from animal.
e. It is blood mix with saline.
37.
5. Transfusion Reactionare
a. Always haemolytic
b. Never haemolytic
c. Can be haemolytic
d. Never febrile
e. Never associated with vomiting.

![ABO blood group System
Phenotype Genotype Antigen Antibodies Frequency (%)
O OO O Anti-A, Anti-B 46
A AA or AO A Anti-B 42
B BB or BO B Anti-A 9
AB AB AB None 3
Rhesus System
The Rhesus D [Rh(D)] antigen is strongly antigenic.
Antibodies to the D antigen are not naturally present in the serum of the
remaining 15% of individuals but their formation may be stimulated by the
transfusion of Rh-positive red cells or they may be acquired during delivery of
a Rh(D) positive baby.](https://image.slidesharecdn.com/6-shockpartiibloodtransfusion-130207001141-phpapp02/85/6-shockblood-transfusion-22-320.jpg)




















































![Blood and Blood Products [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bloodandbloodproductsautosaved-240901181530-603e8a40-thumbnail.jpg?width=640&height=640&fit=bounds)























