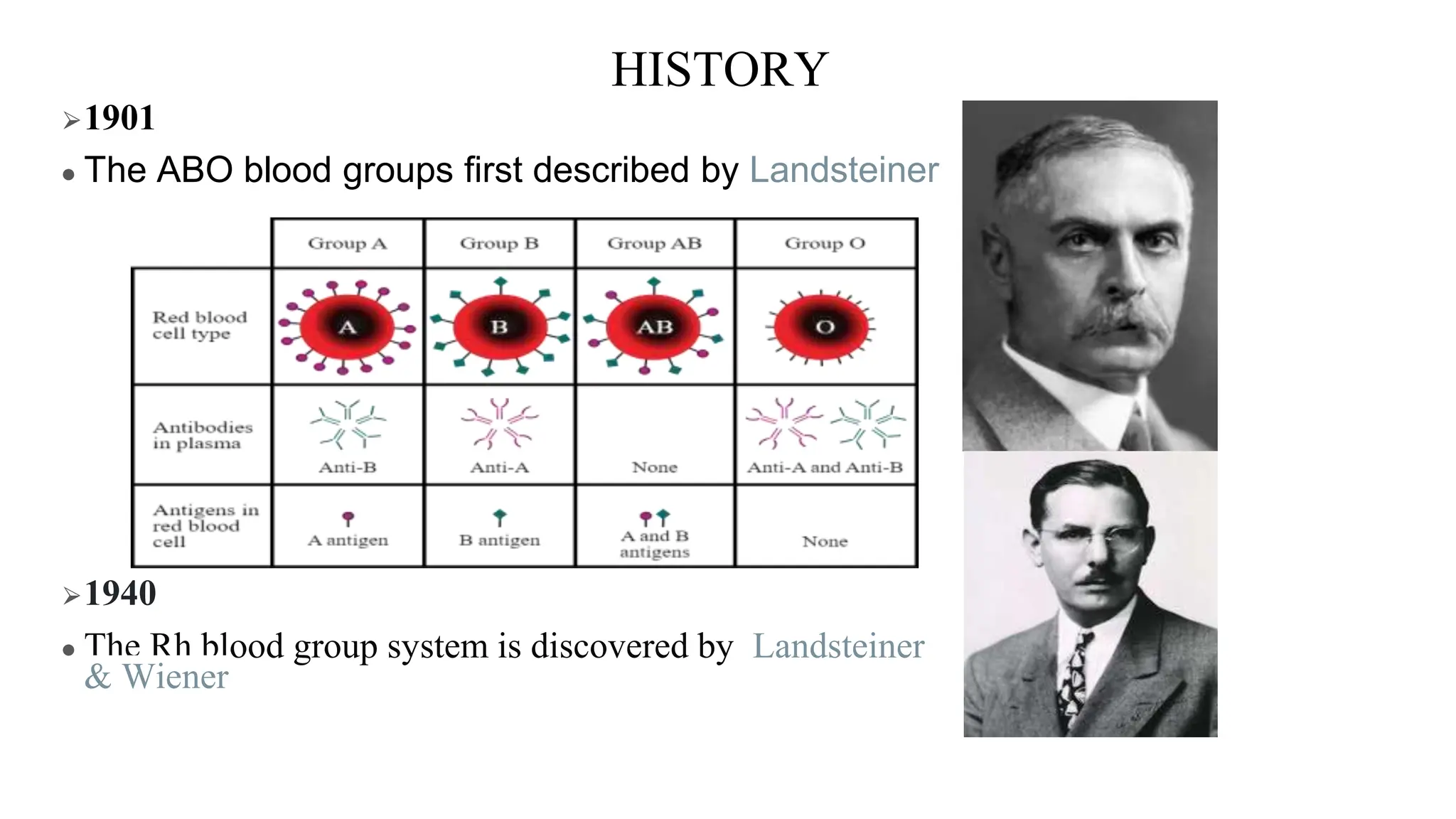
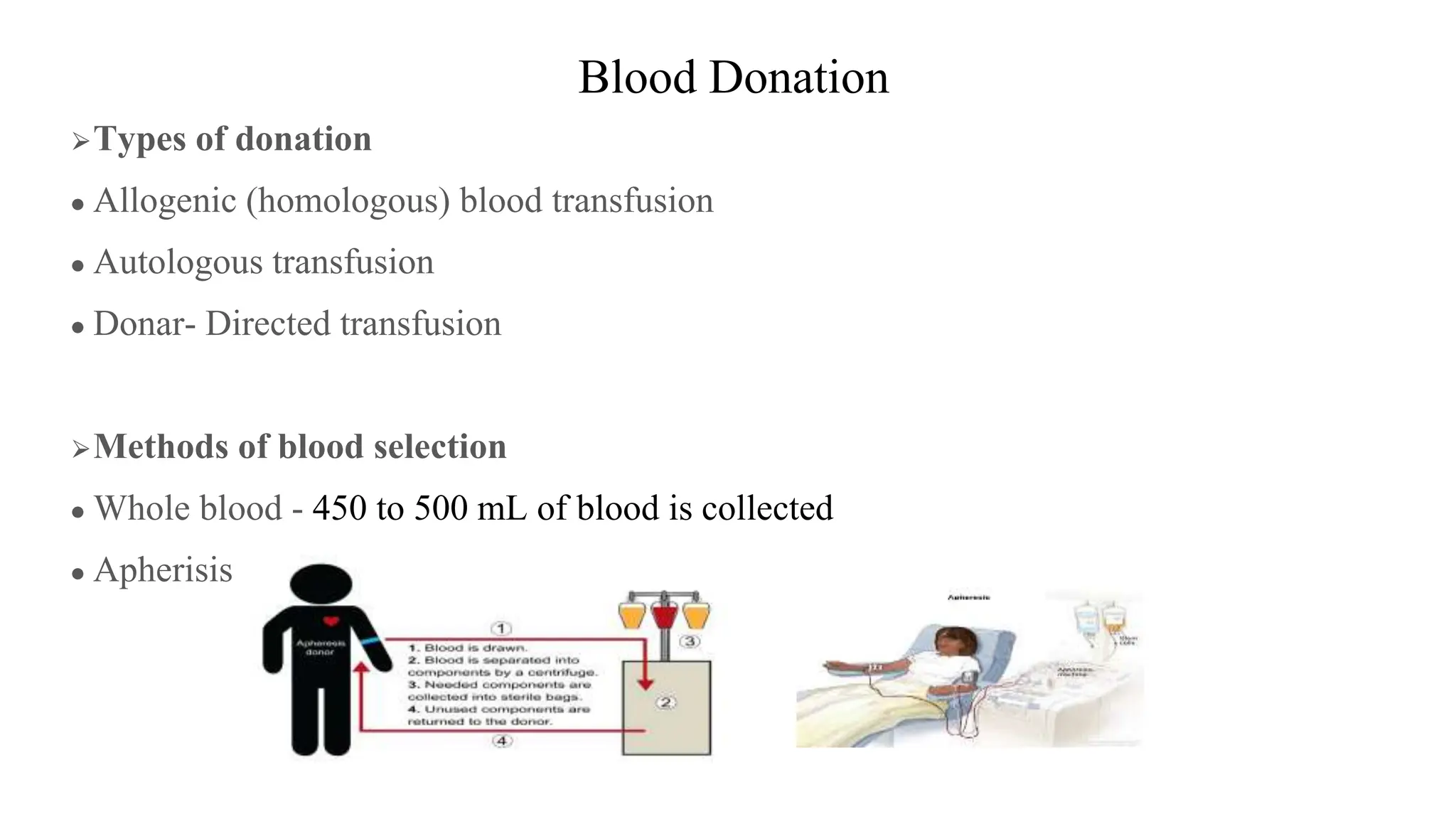
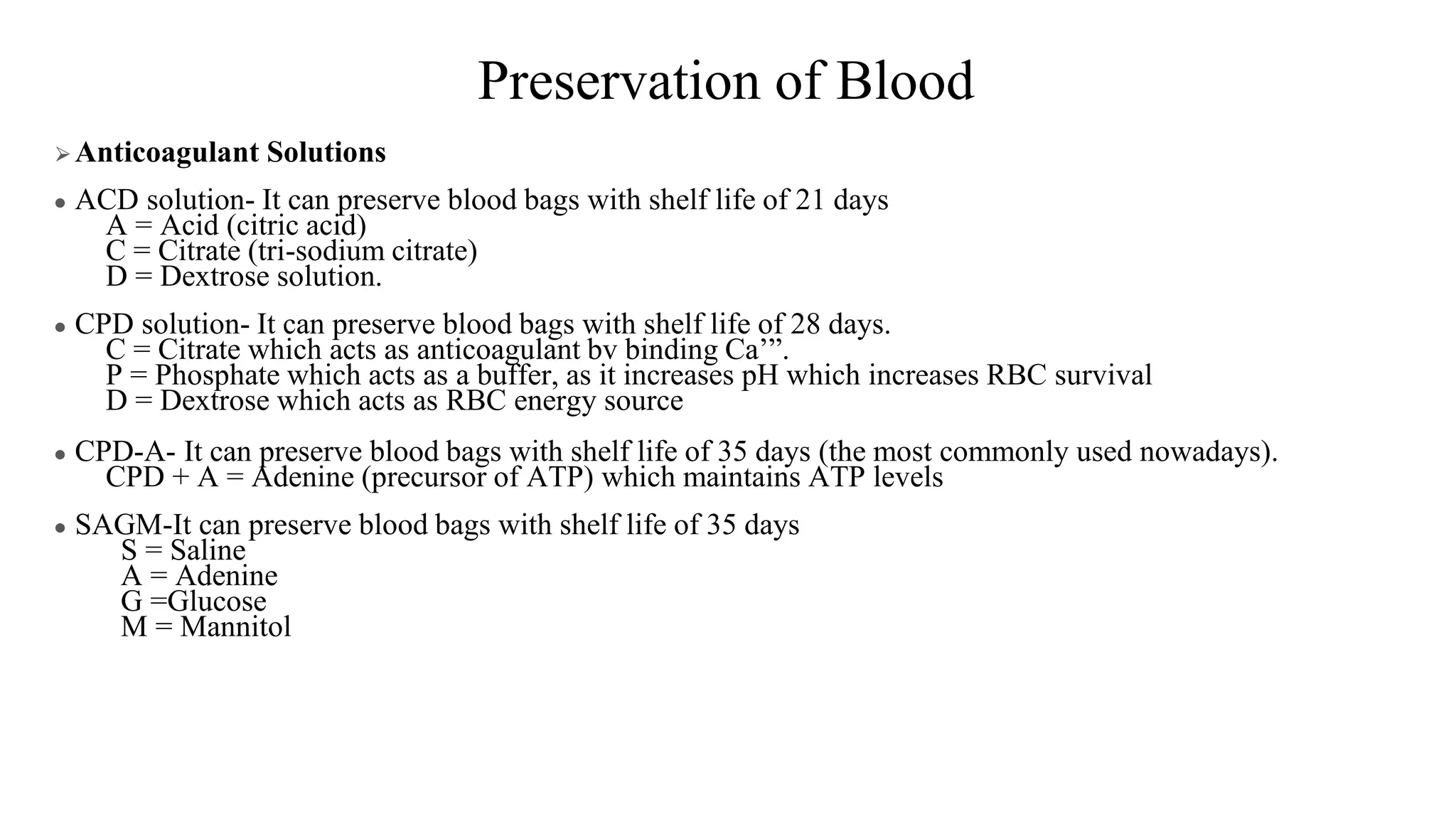
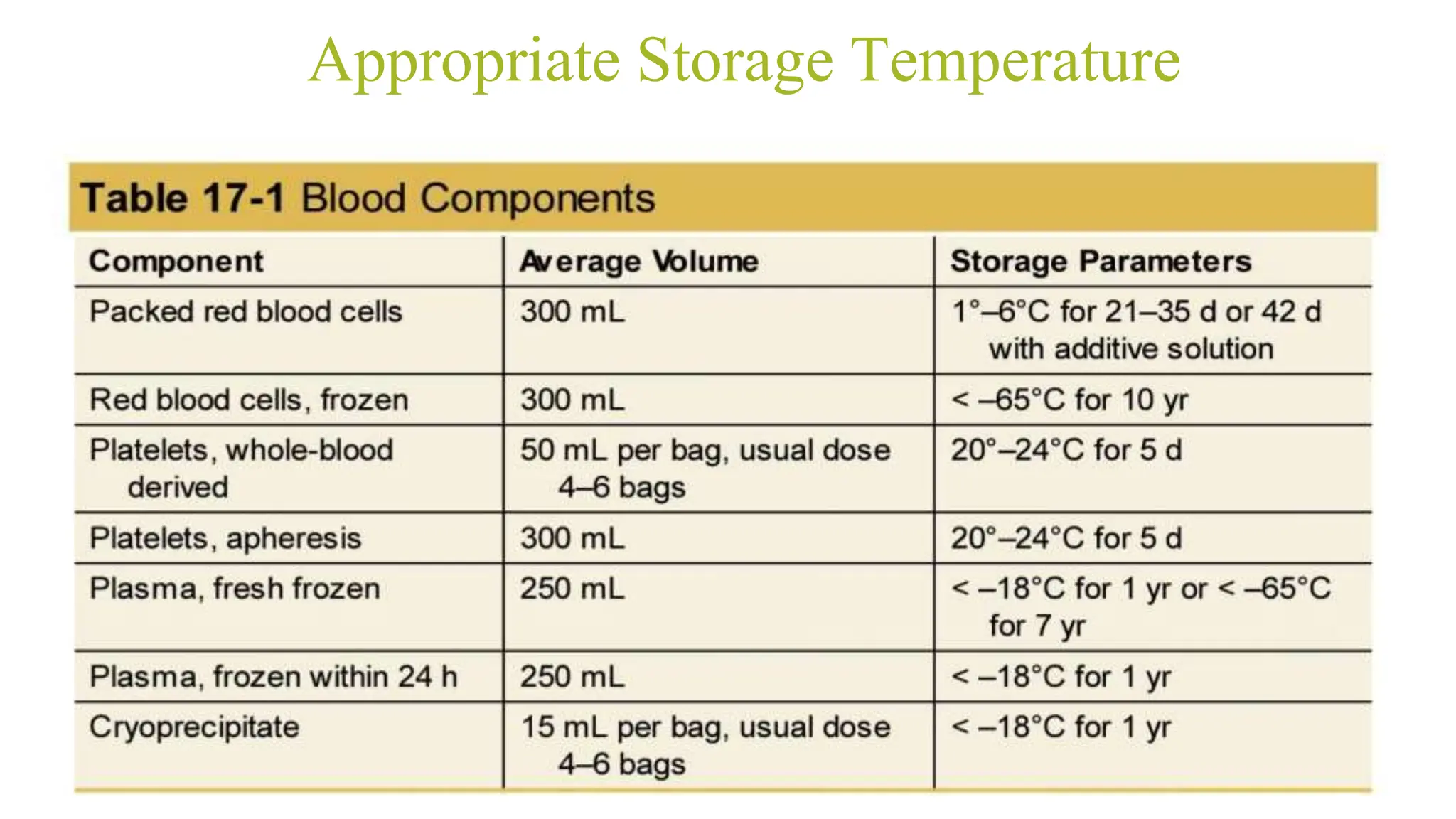
The document provides a comprehensive overview of blood transfusion history, methods, and types of blood components, emphasizing key milestones and landmark discoveries in the field. It outlines the procedures for blood donation, storage, preparation, and transfusion practices, including recommendations for various blood products like packed red blood cells and fresh frozen plasma. Additionally, it discusses the risks associated with blood transfusions, compatibility testing, and blood conservation techniques to enhance patient outcomes.








































![ACUTE NORMOVOLEMIC HEMODILUTION.
● Normovolaemic haemodilution involves removing a patient’s blood and
replacing it with crystalloid to maintain intravascular volume.
● The haematocrit is low; tissue perfusion and blood flow are high due to low
plasma viscosity.
● Blood loss intraoperatively will contain fewer RBCs. Once the blood loss has
stopped, the patient’s own blood can then be returned.
● Volume to be removed = EBV × [(Hcti – Hctt)/Hctave]
● ANH is most effective in patients with high preoperative hemoglobin levels,
minimal cardiovascular comorbidities that allow intraoperative anemia, and a
surgical risk for largevolume blood loss.](https://image.slidesharecdn.com/blood2-240730140346-9b85e09f/75/BLOOD-COMPONENTS-AND-BLOOD-TRANSFUSION-pptx-55-2048.jpg)


















![Blood and Blood Products [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bloodandbloodproductsautosaved-240901181530-603e8a40-thumbnail.jpg?width=640&height=640&fit=bounds)


























![The Post anesthesia care unit [PACU] ppt](https://cdn.slidesharecdn.com/ss_thumbnails/postanaesthesiacareunit-240424172213-667289dc-thumbnail.jpg?width=640&height=640&fit=bounds)

























