Download to read offline



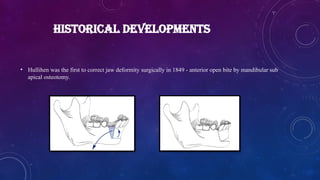
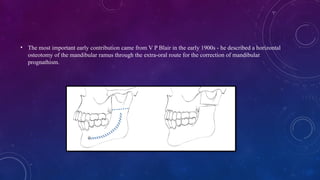

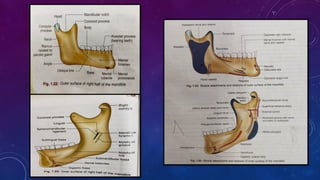
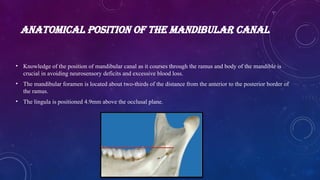
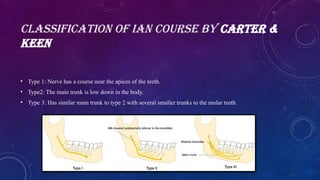


























Introduction Face forms the identity of an individual .Facial deformities invariably make an individual highly self conscious of this abnormal features . The appearance sometimes has a psychological impact on the individual. Definition • The word orthognathic comes from the Greek word “ORTHOS’’ meaning to straighten and ‘’ GNATHOS’’ meaning jaw. • It involves ‘surgical manipulation of the elements of the facial skeleton to restore the proper anatomic and functional relationship in patients with dentofacial and skeletal deformities. HISTORICAL DEVELOPMENTS • Hullihen was the first to correct jaw deformity surgically in 1849 - anterior open bite by mandibular sub apical osteotomy. • The most important early contribution came from V P Blair in the early 1900s - he described a horizontal osteotomy of the mandibular ramus through the extra-oral route for the correction of mandibular prognathism. • Trauner 1955 described the inverted ‘L’ osteotomy of the ramus for the correction of mandibular prognathism. • Caldwell and colleagues modification of L osteotomy to C - osteotomy • Hugo Obwegesser (1955) described the technique of intraoral sagittal split osteotomy for the correction of mandibular problems. • Heinz Köle described the procedure of genioplasty 1968 and a technique to correct open bite. • Burstone et al (1978 & 1980) gave an analysis for the assessment of dentofacial deformity using cephalometric radiographs " The cephalometric analysis for orthognathic surgery" (COGS). • The latest developments in orthognathic surgery is the use of adjunct plastic surgical procedures like liposuction, lip correction. Etiopathogenesis CONGENITAL • Genetic – Underlying genetic predisposition • Syndromes –Apert’s and Crouzon’s syndrome ACQUIRED • Traumatic • Others – neoplastic growth in the jaws, surgical resections etc. Anatomical position of the mandibular canal • Knowledge of the position of mandibular canal as it courses through the ramus and body of the mandible is crucial in avoiding neurosensory deficits and excessive blood loss. • The mandibular foramen is located about two-thirds of the distance from the anterior to the posterior border of the ramus. • The lingula is positioned 4.9mm above the occlusal plane. Classification of IAN course by CARTER & KEEN • Type 1: Nerve has a course near the apices of the teeth. • Type2: The main trunk is low down in the body. • Type 3: Has similar main trunk to type 2 with several smaller trunks to the molar teeth. TIMING OF OSTEOTOMIES • The treatment of dentofacial deformities is based on a careful co-ordination of orthodontics and surgeon. • Early treatment using functional appliances and by orthodontic teeth movements may prevent functional and psychological problems, limit the deformity, shorten treatment time, improve results and obtain stability. • As a rule it is better to wait till the skeletal growth is completed before doing orthognathic surgery.

































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









