
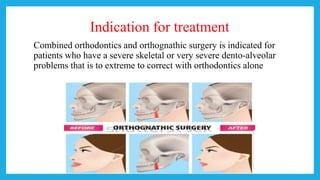
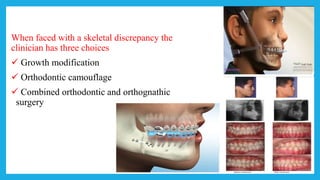





















The document discusses orthognathic surgery, outlining its objectives, indications, contraindications, and treatment planning processes necessary for correcting jaw and facial deformities. Key sections cover various surgical procedures, potential complications, and post-operative care to ensure healing and optimal outcomes. The importance of combined orthodontics and oral surgery is emphasized for patients with severe skeletal or dental issues.
















































































