Downloaded 977 times












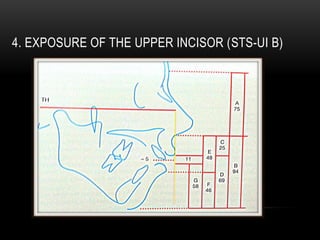
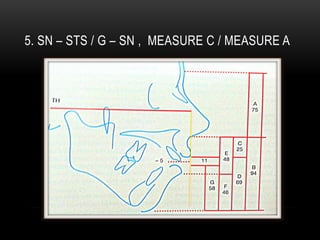
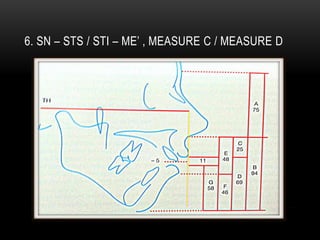

This document discusses cephalometric analysis for orthognathic surgery planning. It outlines landmarks used in the soft tissue analysis and describes horizontal and vertical measurements taken. Key measurements include facial convexity, upper lip length, interlabial distance, and exposure of the upper incisors. The analysis evaluates both hard and soft tissues to determine jaw positions and ensure facial harmony after surgery. Soft tissue considerations are paramount for achieving the primary goal of facial improvement with orthognathic procedures.









































































