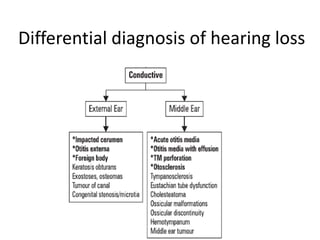
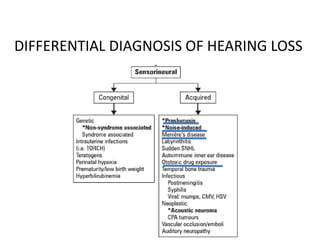
This document discusses hearing impairment, including definitions, types, tests used for diagnosis, and treatment options. It defines the main types of hearing loss as conductive, sensorineural, and mixed. Diagnosis involves a medical history, physical exam, and tests like pure tone audiometry, tympanometry, and auditory brainstem response testing. Treatment depends on the underlying cause but may include medications, surgery, hearing aids, or cochlear implants. Regular screening is important due to the high prevalence of hearing loss.












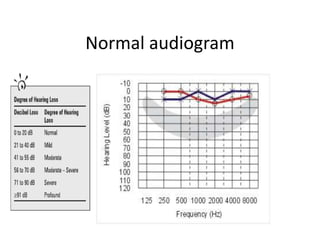
![Pure tone audiometry (PTA)
• PTA is the key hearing test used to identify
hearing threshold level of an individual, enabling
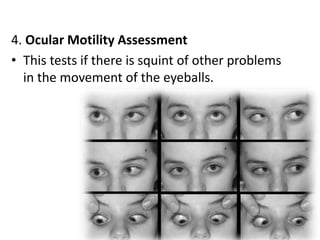
determination of the degree, types and
configuration of hearing loss.
• Provides the basis for diagnosis and management.
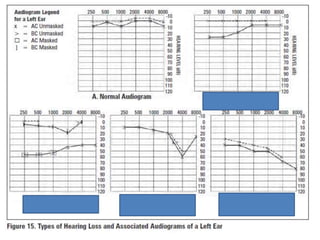
• The symbols used on most audiograms are:
– x - left, air conduction
– o - right, air conduction
– ] - left, bone conduction
– [ - right, bone conduction](https://image.slidesharecdn.com/vwmkjpymr92jyr7wfyle-signature-49daf8f7362d363afe9c306603fb1bcfbac832a92e8fdb001f22a27835c798e9-poli-160528123706/85/5-visual-hearing-impairment-62-320.jpg)