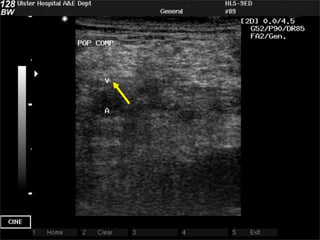
Compression ultrasound of the legs can detect deep vein thrombosis (DVT). Key sites to compress include the femoral vein in the groin, the femoral vein just above the knee, and the below knee veins which can be visualized from the front of the leg between the tibia and fibula. Compressing the veins and looking for non-compressibility is the gold standard for diagnosing DVT on ultrasound. Scanning multiple sites increases sensitivity but can be more irritating for patients.