Venous thrombosis
• Mostcommon direct cause of death in surgical patients.
• Formation of a semisolid coagulum within venous
system and may occur in superficial system (SVT or
‘thrombophlebitis’) or deep system (DVT).
• Immediate risk of pulmonary embolus and sudden death.
• Risk of developing PTS and venous ulceration.
• DVT may occur in the upper limb also but complications
and morbidity more in leg DVT
3.
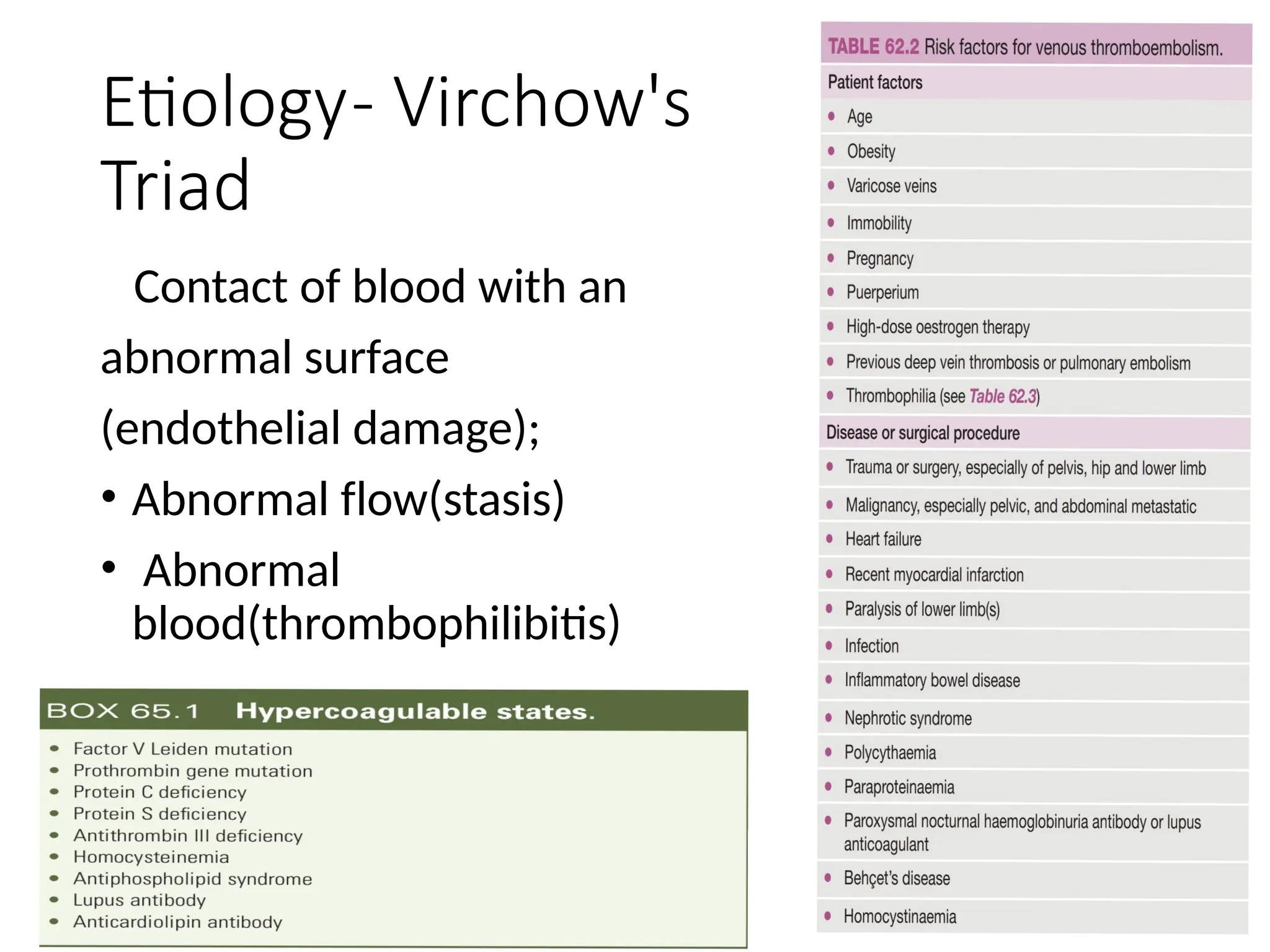
Etiology- Virchow's
Triad
Contact ofblood with an
abnormal surface
(endothelial damage);
• Abnormal flow(stasis)
• Abnormal
blood(thrombophilibitis)
4.
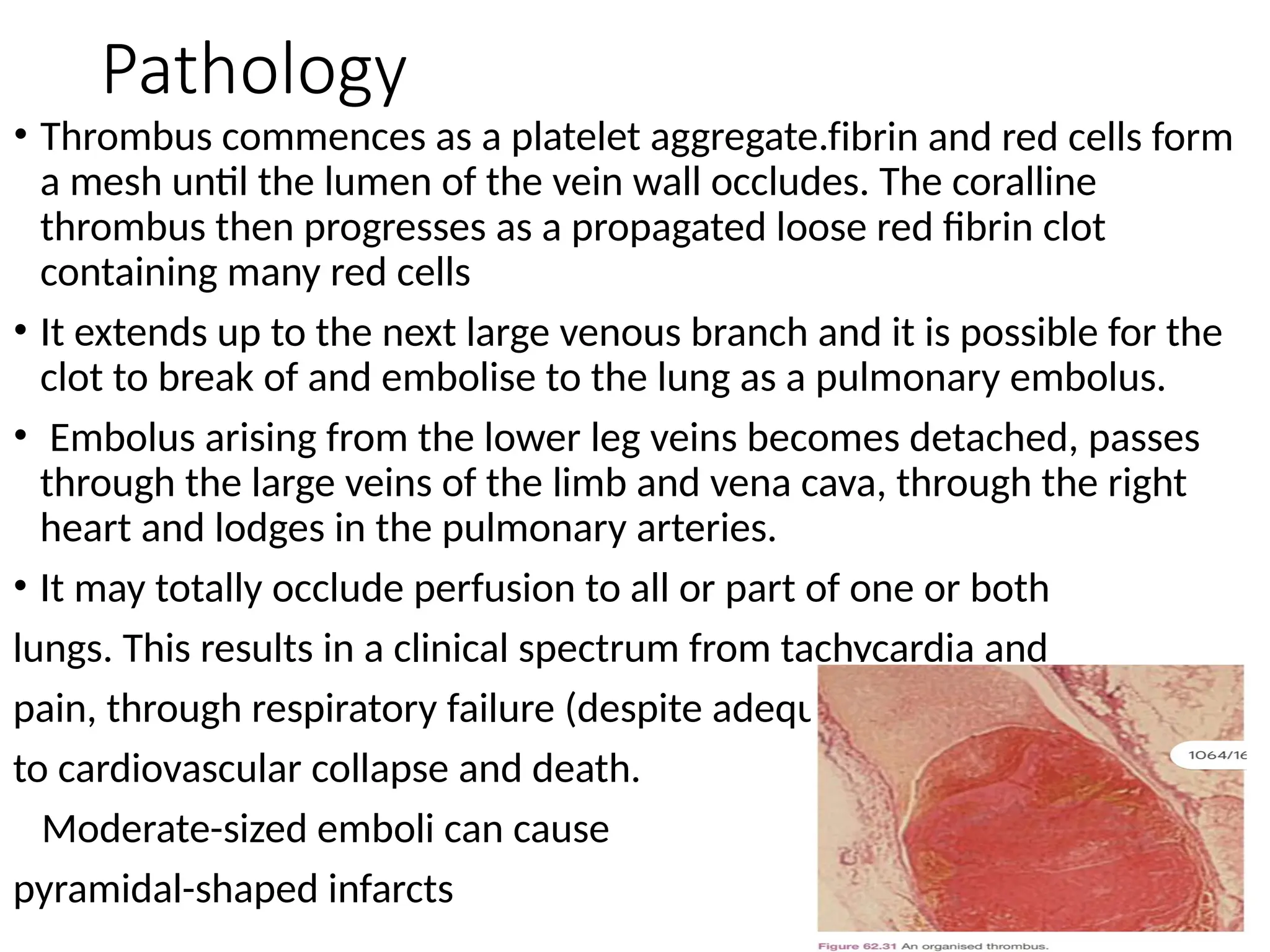
Pathology
• Thrombus commencesas a platelet aggregate.fibrin and red cells form
a mesh until the lumen of the vein wall occludes. The coralline
thrombus then progresses as a propagated loose red fibrin clot
containing many red cells
• It extends up to the next large venous branch and it is possible for the
clot to break of and embolise to the lung as a pulmonary embolus.
• Embolus arising from the lower leg veins becomes detached, passes
through the large veins of the limb and vena cava, through the right
heart and lodges in the pulmonary arteries.
• It may totally occlude perfusion to all or part of one or both
lungs. This results in a clinical spectrum from tachycardia and
pain, through respiratory failure (despite adequate ventilation)
to cardiovascular collapse and death.
Moderate-sized emboli can cause
pyramidal-shaped infarcts
5.
Investigations
• VENOGRAPHY
• Injectionof contrast material into the venous system
• The superficial venous system has to be occluded with a
tourniquet, and the veins in the foot are injected for
visualization of the deep venous system.
• invasive,subjects to risks of IV administration of contrast
material.
• Has been replaced by less
invasive modalities.
6.
Impedance Plethysmography
• Measuresthe change in venous capacitance and rate of
emptying of the venous volume on temporary occlusion and
release of the occlusion of the venous system.
• A cuff is inflated around the upper thigh until the electrical
signal has plateaued. When the cuff is deflated, there is
usually rapid outflow and reduction of volume.
• With a venous thrombosis, one notes a prolongation of the
outflow wave.
• It is not useful clinically for the detection of calf venous
thrombosis and of patients with prior venous thrombosis.
7.
Fibrin and FibrinogenAssays
• Fibrin and fibrinogen levels can be determined by
measuring the degradation of intravascular fibrin.
• The D-dimer test measures cross-linked degradation
products, which is a surrogate of plasmin’s activity on
fibrin. In combination with clinical evaluation and
assessment, the sensitivity exceeds 90% to 95%.
Modified Wells criteria
8.
Duplex ultrasound
• Currenttest of choice for the diagnosis of DVT is duplex
ultrasound, it combines Doppler ultrasound and color flow
imaging.
• Advantage of this test is that it is noninvasive, comprehensive,
and without any risk of reaction to contrast angiography
• It evaluates flow with distal compression, which results in
augmentation of flow, and with proximal compression, which
should interrupt flow.
• If any segment of the venous system being examined fails to
demonstrate augmentation on compression, venous thrombosis
is suspected
• The probe is also used to compress the vein.
• A normal vein is easily compressed, whereas in the presence of
a thrombus, there is resistance to compression.
9.
MRVI
It is auseful test for imaging the iliac veins and IVC, an area
where the use of duplex ultrasound is limited.
MRVI is less invasive than conventional venography and is
able to directly visualize the thrombus.
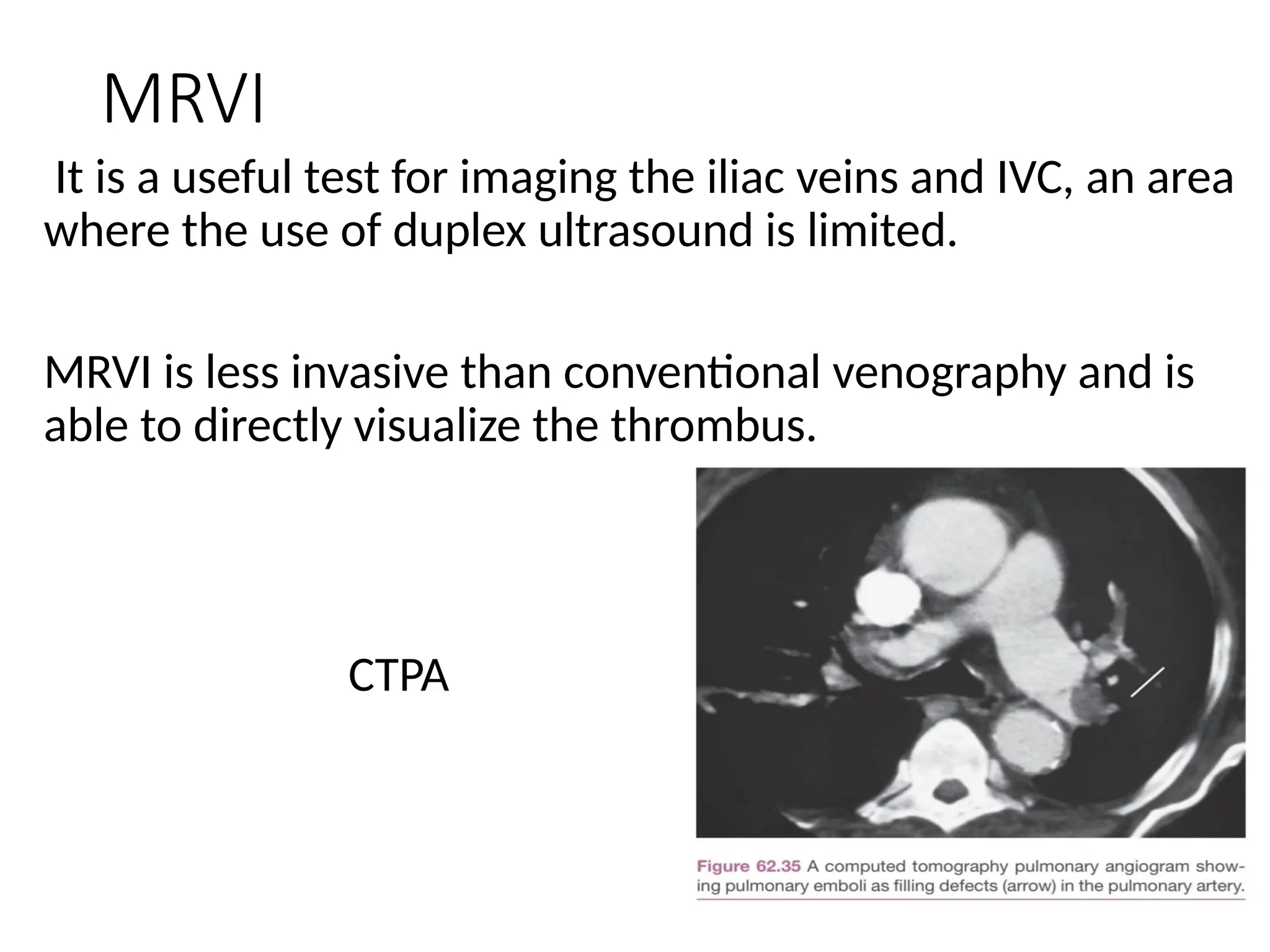
CTPA
10.
DDs
• The diferentialdiagnosis of a DVT includes a
• ruptured Baker’s cyst,
• calf muscle haematoma
• ruptured plantaris muscle
• thrombosed popliteal aneurysm
• arterial ischaemia
11.
Prophylaxis
• patient undergonemajor abdominal or orthopedic surgery,
has sustained major trauma, or has prolonged immobility
(>3 days) represents an elevated risk for the development
of venous thromboembolism.
• The methods of prophylaxis can be mechanical or
pharmacologic.
• Simplest method is for the patient to walk within 24 to 48
hours. Activation of the calf pump mechanism is an
effective means of prophylaxis.
• Most common method of surgical prophylaxis is sequential
compression devices, which periodically compress the
calves and essentially replicate the calf bellows
mechanism.
• They prevent venous stasis and increase fibrinolytic activity
12.
Prophylaxis
• 5000 unitsof unfractionated heparin every 8 hours sc.
Patients in the medium- or high-risk groups should be
considered for pharmacological prophylaxis
13.
Treatment
• Any venousthrombosis involving the femoropopliteal
system is treated with full anticoagulation.
• The treatment of DVT has centered around heparin
treatment to maintain the PTT at 60 to 80 seconds,
followed by warfarin therapy to obtain an INR of 2.5 to 3.0.
• An initial bolus of 80 units/kg or 5000 units IV bolus is
administered, followed by 18 units/kg/hr.
• Warfarin is started on the same day.
• If warfarin is initiated without heparin, the risk for a
transient hypercoagulable state exists because protein C
and protein S levels fall before the other vitamin K–
dependent factors are depleted
14.
Anticoagulation
• A minimumtreatment time of three months is advocated in most cases.
• If the patient has a known hypercoagulable state or has experienced
episodes of venous thrombosis, however, lifetime anticoagulation is
required in the absence of contraindications.
• Oral anticoagulants are teratogenic and thus cannot be used during
pregnancy. In the case of the pregnant patient with venous thrombosis,
LMWH is the treatment of choice; this is continued through delivery and
can be continued postpartum, as indicated.
• Oral anticoagulation using new or ‘novel’ anticoagulants (NOACs), which
directly inhibit either factor Xa (rivaroxaban
and apixaban) or thrombin (dabigatran), is recommended as
they are equally efective as vitamin K antagonists (warfarin)
in preventing recurrent symptomatic VTE but are associated
with less major bleeding complications.
15.
Catheter directed thrombolysis
•The purported benefit is preservation of valve
function, with a subsequently lesser chance for
development of PTS
• Based on the result of the ATTRACT (Acute Venous
Thrombosis: Thrombus Removal with Adjunctive
Catheter-Directed Thrombolysis) Trial, catheter
directed thrombolysis may be recommended in
patients with a more proximal, iliofemoral
involvement and moderate to severe symptoms.
16.
Endovascular reconstruction
• Chronicproximal venous occlusion of the iliofemoral system
is a challenging clinical problem
• Recanalization of the occluded iliac vein is performed
endovascularly. Balloon dilation of the lesion is then
performed, and a stent is placed across the dilated segment
PULMONARY EMBOLUS
• Most pulmonary emboli can be treated by anticoagulation
and observation, but severe right heart strain and shortness
of breath indicate the need for thrombolysis or
radiologically guided catheter embolectomy.
17.
Upper extremity DVT
•Upper extremity DVT is much less common than its lower extremity
counterpart
• Pulmonary embolism occurs in up to one third of all patients with an
upper extremity DVT.
• Upper extremity DVT usually refers to thrombosis of the axillary or
subclavian veins.
• The syndrome can be divided into two categories, primary idiopathic
and secondary
• Primary causes include Paget-Schroetter syndrome and idiopathic
upper extremity DVT.
• Patients with Paget-Schroetter syndrome develop effort thrombosis
of the extremity caused by compression of the subclavian vein, the
venous component of thoracic outlet syndrome
A classic presentation involves a young athlete who uses the upper
extremity in a repetitive motion, such as swimming, which causes
repetitive extrinsic compression of the subclavian vein.
18.
Upper extremity DVT
•In these patients, anatomic anomalies such as a
cervical rib or myofascial bands cause the venous
compression.
• Plain films are one of the first diagnostic tests used to
confirm thoracic outlet syndrome.
• Treatment with initial thrombolysis followed by
thoracic outlet decompression (anterior and middle
scalene resection, first rib resection) with possible
balloon angioplasty or surgical reconstruction of the
axillary and subclavian veins is the standard of care.
19.
Cont
• Idiopathic upperextremity DVT is sometimes eventually
attributed to an occult malignant neoplasm, and therefore
a diagnosis of idiopathic upper extremity DVT warrants
evaluation for an undetected malignant neoplasm.
• Secondary causes of upper extremity DVT include an
indwelling central venous catheter, pacemaker,
thrombophilia, and malignant disease.
• Classic findings on physical examination include unilateral
swelling, pain, extremity discomfort, erythema, and a
palpable cord.
• Diagnosis is confirmed by duplex ultrasonography.
Because the clavicle obscures the midportion of the
subclavian vein, venography or magnetic resonance
venography may be required
20.
Treatment
• Treatment ofupper extremity DVT involves anticoagulation
therapy.
• Therapeutic dosing parameters are the same as for lower
extremity DVT.
• Treatment should be for 3 months and consist of heparin or
LMWH plus warfarin for at least 3 months.
Ivc filters
21.
SUPERFICIAL THROMBOPHLEBITIS
• Cardinalsigns of a superficial thrombophlebitis are rubor,
calor, dolor, and, tumor describing a linear, erythematous,
tender, and swollen lesion along the course of a superficial
vein.
• The condition is self-limiting in the majority of patients and
as result of the inflammatory reaction,the superficial vein
becomes a palpable fibrotic cord.
• In hospitalized patients, superficial thrombophlebitis is
usually caused by an indwelling catheter.
• The common predisposing risk factors are recent surgery,
recent childbirth, venous stasis, varicose veins, or IV drug
use
22.
Superficial thrombophlebitis
• In1876, Trousseau identified the phenomenon of
migratory thrombophlebitis and malignant disease,
particularly involving the tail of the pancreas.
• Diagnosis made by physical examination of an
erythematous palpable cord coursing along a superficial
vein, usually located along the lower extremities.
• Duplex ultrasonography is recommended to confirm
diagnosis
23.
Treatment
• The initialtreatment of localized noncomplicated
thrombophlebitis involves conservative therapy,
which consists of antiinflammatory medication and
compression stockings.
• The recommended treatment of a superficial
thrombophlebitis, involving a ≥5 cm great
saphenous vein segment is a midtreatment dose of
LMWH (enoxaparin 60 mg daily subcutaneously) or
fondaparinux (2.5 mg daily subcutaneously) for a 6-
week period